This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transitioning from working as an ICU nurse to becoming a Certified Registered NurseAnesthetist (CRNA) is a journey marked by immense growth but also profound challenges. Understanding the Shift The transition from ICU to operating room (OR) involves a fundamental change in responsibilities.
What’s the difference between a physician anesthesiologist and a nurseanesthetist? After the first 3 – 4 years in the workforce, either one can master the manual skills of anesthesia. So what really is the difference between a physician anesthesiologist and a nurseanesthetist? The answer: internal medicine.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
Pre-operative anxiety , the psychological distress which patients experience that is provoked by concerns related to their surgical and anesthetic care, 1 is estimated to affect up to 75% of children 2 and 80% of adult patients. 3,4 It has been linked to multiple intra-operative and post-operative complications (e.g.,
In the smart glasses group, the ultrasound machine was located behind the operator, and the smart glasses were paired with the ultrasound machine. Would the addition of smart glasses for routine monitoring be an overdose of technology in the operating room cockpit? The physician medical literature has not studied the issue.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operating rooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operating room supplies. The video is posted here. The required parts are an operating room anesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps.
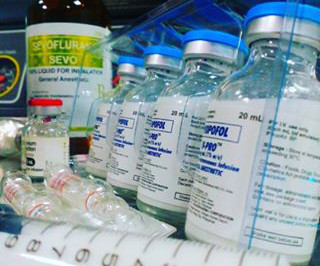
Anesthesiologists still work in hospital operating rooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. The job of a certified nurseanesthetist was listed as #11 on the Best Paying Jobs list. What Are the Common Anesthesia Medications?
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered NurseAnesthetists). Why did this change happen?
Advanced Practice Provider Spotlight: Certified registered nurseanesthetist shares perspective on caring for diverse patients Posted April 11, 2023 by ,Penn State Health News Prolung Ngin , a certified registered nurseanesthetist (CRNA) at Penn State Health Milton S.
Certified Registered NurseAnesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. Anesthesia is a vital tool in modern medicine and CRNAs serve as experts in providing this medical service to patients. To begin, it’s essential to understand the role of a CRNA.
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurseanesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists win the tally for most operating room hours per week.
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
Introduction: In the ever-evolving landscape of healthcare, understanding the dynamics of the anesthesia labor market is crucial for healthcare organizations striving to recruit and retain top talent. Don’t miss this opportunity to stay ahead in understanding the anesthesia labor market landscape.
Salem Anesthesia is fortunate to have the best Anesthesiologists on our team. Additionally, the anesthesiologist leads teams of certified registered nurseanesthetists ( CRNA s) and certified anesthesiologist assistants (CAAs). Salem Anesthesia truly values the remarkable anesthesiologists in our group!
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From General Anesthesia?
million operations from taking place (3). An aging population has correlated with an increasing demand for surgical and anesthesia services that has outpaced the number of anesthesiologists entering the profession (5). ASA Monitor , January 2022, [link] “The Anesthesia Provider Shortage.”
More care team anesthesia and more Certified NurseAnesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. Anesthesia has never been safer.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). The scrubs are enclosed in a device not dissimilar to a soda machine, and you need your ID to operate it. Empty Operating Room 0655 hours—You don a bouffant hat and a facemask, and enter your operating room.
Point/Counterpoint: How new is modern anesthesia? Are modern anesthesia techniques radically different from the methods of twenty years ago? How can it be that general anesthesia has ceased to evolve? What about regional anesthesia? Anesthesia in 2018 is markedly different from anesthesia in the 1990s.
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. Nurses consistently have their backs to patients as they type, type, type data into computer terminals.
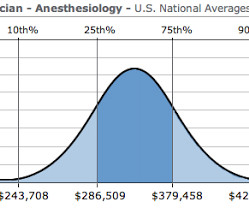
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
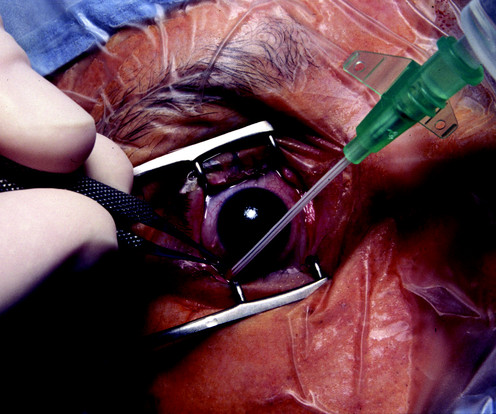
You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists. You are on call for the repair. What do you do? Discussion: There are two issues.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
The only way to end the sedative effects of propofol is for an anesthesia professional to support the airway, breathing, and circulation of the patient until the drug effects of propofol wear off in time. I’ve never administered a dose of flumazenil in my entire career, nor have most of my anesthesia colleagues.
My aim is to inform my readers, both anesthesia professionals and laypersons, that if Medicare for All becomes reality, there will be a dire consequence regarding anesthesia staffing and services to patients. What happens if every anesthesia patient pays only Medicare rates in a Medicare for All future? 75 X $76) + (.25
Let me begin by offering two anecdotes: I was an invited visiting anesthesia professor at a major university this year, and following one of my lectures an anesthesiology resident approached me for a discussion. The demand for anesthesia services will grow. How much money does an anesthesiologist earn? It depends.
I commonly hear two questions from my patients: “How does anesthesia work?” General anesthesia is the sum of hypnosis (sleep), amnesia, analgesia (pain relief), and the lack of any motion response to pain. Why Did Take Me So Long To Wake From General Anesthesia? Will I Have a Breathing Tube During Anesthesia?
An anesthesia colleague wrote to me several months ago, asking for my recommendations for achieving smooth emergence. In each of these surgeries, the surgeon has an intense interest in a gentle anesthesia wake-up, free of coughing, bucking, or hypertension. His question prompted me to write this column. to 25 μg/kg/hr.”
Nowadays when patients arrive at the hospital for surgery, it’s not uncommon for them to be armed with abundant information on their disease, their pending operation, and even their anesthesia options. Anyone can put medical information on a Web server, and the information posted may be incorrect or outdated.
Anesthetist options were limited. Before her surgery, Alexandra reclined awake on the operating room table. About one patient out of ten is nauseated after anesthesia. I stood at the anesthesia workstation and reviewed my checklist. Life is a series of choices. I chose to be my wife’s doctor. These are the common risks.
Anesthesiology is a wonderful profession, as I have described in many previous posts on theanesthesiaconsultant.com. But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. In the operating rooms, the patients are brought in by the surgeons. What is this threat?
Anesthesia is a hands-on specialty. Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operating room. Since the development of the internet, anesthesia practice has changed forever.
This technique induced vasoconstriction and resulted in decreased blood loss, and made transfusion and post-operative anemia rare. The procedures are done under general endotracheal anesthesia, and can last from 3 to 8 hours. Our facility, the Plastic Surgery Center in Palo Alto, has two operating rooms.
Louis Imagine this: You’re an anesthesiologist in the operating room at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger.
See Robot Anesthesia and Robot Anesthesia II ) AI already influences our daily life. Anesthesiologists work in operating rooms and intensive care units—acute care settings which demand vigilance, steady hands, and quick thinking. I’m fascinated by the topic of artificial intelligence in medicine. I can’t wait to see it.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. The patient consents.
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. INTRAOPERATIVE DECISION A 60-year-old man with a history of hypertension is having a knee arthroscopy surgery under general anesthesia. This could indicate a cardiac event or a complication related to the anesthesia.
He writes, “Our specialty, anesthesia, has suffered an identity crisis for decades. In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operating room. Read my column on bullying in the operating room. Hold your heads high.
The most difficult challenge for any anesthesiologist is the transition from the end of anesthesia residency into the beginning of your first job. Their role is to teach anesthesia, to take care of patients, and to do research. Why are jobs posted on Internet sites usually inferior jobs? They are not guidance counselors.
Surgeons, anesthesiologists, certified nurseanesthetists, and operating room nurses are barely working at all now, for the fourth consecutive week. The post UNDEREMPLOYED: AMERICAN SURGEONS, ANESTHESIOLOGISTS AND NURSES appeared first on The anesthesia consultant.
How do you feel when you meet your anesthesia provider prior to a surgical procedure? In an abstract presented at the 2015 American Society of Anesthesiologists annual meeting, data from the 2014 National Anesthesia Clinical Outcomes Registry was compiled for every anesthesiologist of known age who performed at least 100 cases.
Every anesthesia provider must learn to free-solo anesthesia early in his or her career. A typical hospital will have dozens of other anesthesia providers working in the same building. Commercial aviation is sometimes compared to anesthesia practice. In anesthesia there is no guaranteed second anesthesiologist.
An anesthesia residency is three years long, preceded by one year of internship. One year after medical school, the same graduate who just completed twelve months of internship now reaches perhaps an even more difficult transition—the first months of anesthesia residency. After ten minutes, he left to pursue other duties.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content