This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Perioperative hypothermia, defined as a core body temperature below 36°C, is a frequent and preventable complication associated with anesthesia and surgical procedures. The post-operative phase is crucial for reinforcing normothermia and supporting patient recovery, yet it is often overlooked in thermal management.
Post-AnesthesiaCare Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operating room and continues until they are stable enough to recover at home or in a hospital room. PACU nurses contribute significantly to this efficiency.
Here are five warning signs that your anesthesia team might be underperforming: 1. Clinical Inefficiencies Clinical inefficiencies can manifest as non-compliance with internal and external standards, policies, procedures, and best practices. Lookout for: A trend toward severe post-operative nausea and vomiting.
The main questions as to whether a hospital or an ambulatory surgery center can resume elective surgery as of May 2020 are: What is the incidence of COVID-19 in your geographic area? When I’m at Stanford Hospital or the surgery centers in our area I’m confident the environment is safe.
They play a crucial role in healthcare by ensuring patient safety and comfort before, during, and after surgical procedures. Anesthesia is a vital tool in modern medicine and CRNAs serve as experts in providing this medical service to patients. Proper planning creates the best possibility for surgical procedures to go well.
Sixty-six percent of surgeries in the United States take place as an outpatient , and many of these surgeries are performed at freestanding facilities distant from hospitals. If the patient is unstable, a physician, usually an anesthesiologist, will need to accompany the patient and the EMTs to the hospital emergency room.
Many OSA patients present for non-airway procedures such as orthopedic surgeries, abdominal surgeries, or endoscopies and colonoscopies. Other OSA patients present for procedures designed to improve their sleep apnea. These procedures involve surgical modification of the upper airway.
You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% The patient does well, and is discharged from the PostAnesthesiaCare Unit in excellent condition. The patient objects. Let’s do it.” He’s right.
Yet, with a single minute in the OR costing as much as $120, ASCs, hospital outpatient departments (HOPD), and ORs regularly waste much more than that. The reasons for low OR utilization rates are multifactorial, yet they often trace back to ineffective pre-anesthesia testing processes. Do it again. Wait another minute. It’s unlikely.
To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. You complete your morning bathroom and breakfast routines, and leave your residence at 0630 hours for the hospital. Your hospital contains multiple operating rooms, and today you are in room #10.
It’s not infrequent that autistic patients need surgery and anesthesia. Patients with autism commonly need to be sedated for routine procedures that a normal child or adult would cooperate with. He is verbal with his mother, but refuses to interact with the anesthesia or nursing personnel. mg/kg midazolam, and.02
Lastly, detail specific nursing skills related heart procedures or surgeries that you have experience performing and what responsibilities you've been given by doctors and other healthcare professionals in order to create the best care plan for each patient.
Some were academic professors, some were trainees at a university, and some were community anesthesiologists either in my group or in other anesthesia companies. We’re entering an era of metrics for physicians, in which the government and hospital systems will collect data to monitor quality and performance.
The Barnes Jewish Hospital, Washington University, St. Louis Imagine this: You’re an anesthesiologist in the operating room at a busy hospital. Anesthesiologists at Barnes Jewish Hospital at Washington University in St. Louis, Missouri are studying a novel system they call the Anesthesia Control Tower (ACT).
The anesthesiologist and the operating room nurse transport the patient to the PACU (PostAnesthesiaCare Unit), where the patient is connected to the standard monitors of pulse oximetry, ECG, blood pressure, and temperature. This is every anesthesia provider’s nightmare. per 100,000 outpatient procedures.
One day after attending the ASA meeting in San Francisco, I heard an in-person lecture in Palo Alto, California by Professor Anil Patel from the Royal National Throat, Nose and Ear Hospital in London. I believe many smaller hospitals and outpatient facilities such as ambulatory surgery centers do not own the required equipment.
Tell the surgeon that the patient needs to have cardiac clearance prior to any general anesthetic, and that the case needs to be done in a hospital setting rather than at a freestanding surgery center. Just do MAC (Monitored AnesthesiaCare) anesthesia for this case, but make sure he’s asleep.
In 1999 the Institute of Medicine published the landmark “To Err is Human” report , which described that adverse events occurred in 3 – 4% of all hospital admissions, and that over 50% of the adverse events were due to preventable medical errors. This hampers care improvement. Mistakes happen in medicine.
The audit trail is NOT part of the EMR printout, and it’s not visible on the EMR patient care screen that we healthcare providers see. Lawyers can subpoena the audit trail in malpractice legislation, and the hospital must provide the audit trail if the court decides that the audit trail is relevant.
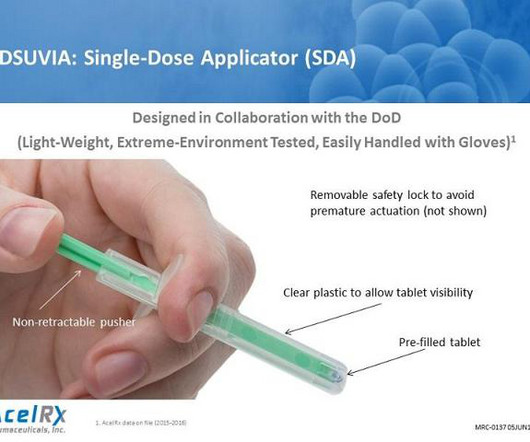
The FDA approved the drug to be used in hospital settings only, for the treatment of moderate-to-severe acute pain, where a narcotic is needed and rapid onset is desired, but the route of administration does not require intravenous access. Typical settings would be the surgical wards after major orthopedic or general surgery procedures.
That would seem to be the essence of anesthesia practice, but you must become more than a technician. Youre a physician who must become expert in all aspects of medical care before, during, and after a surgical procedure. They can watch you for a short period of time while you supervise the safe landing of the anesthesia plane.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content