This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
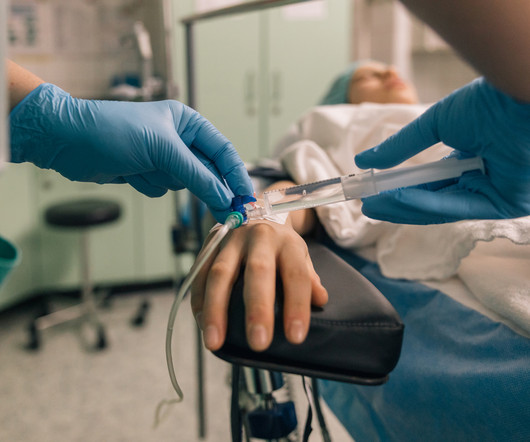
Perioperative hypothermia, defined as a core body temperature below 36°C, is a frequent and preventable complication associated with anesthesia and surgical procedures. Even brief periods of pre-operative warming (ranging from 10 to 15 minutes) can significantly improve intra-operative thermal stability (2).
Rural hospital closures in the United States have become an increasingly concerning trend in recent years, with significant implications for healthcare access and quality in affected communities. Since 2010, over 130 rural hospitals have shut their doors, with a record 19 closures occurring in 2020 alone.
Perioperative Services and Anesthesia success depend on attracting and retaining anesthesia providers at a reasonable cost. Anesthesia providers in most organizations feel undervalued and unappreciated. Organizations that have stable anesthesia coverage have common characteristics contributing to anesthesia satisfaction.
Here are five alarming numbers—and how smarter operational and clinical tools can help. Maintaining financial stability amidst these reductions means improving operational efficiency and ensuring complete charge capture. Analytics platforms offer deep insights into anesthesia staffing models and cost management.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
In the smart glasses group, the ultrasound machine was located behind the operator, and the smart glasses were paired with the ultrasound machine. Would the addition of smart glasses for routine monitoring be an overdose of technology in the operating room cockpit? Does excessive technology distract us from the actual patient?
Luke’s Health System, Robert Eisenberg, RN, MBA, CASC, Senior Vice President, ASC Practice Leader, Sullivan Healthcare Consulting, Nicole Brown, Chief Operating Officer Orthopedics & Sports Medicine, St. Luke’s wanted the surgery center to run with the operational mentality of an ambulatory surgery center (ASC).
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operating rooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
Operating Room (OR) nurses, also known as perioperative nurses, play an essential role in surgeries. OR nurses are the backbone of the operating room, advocating for patients and supporting the entire surgical team. OR nurses are the backbone of the operating room, advocating for patients and supporting the entire surgical team.
Ahead of a visit to the hospital for a surgical procedure, patients often have plenty of questions about what to expect — and can be plenty nervous. These virtual teammates can have natural, human-like conversations with patients, answer a wide range of questions and provide supporting guidance prior to preadmission appointments at hospitals.
Annual meeting Vice-Chair Dr. Engy Said put together a fantastic point-of-care ultrasound and regional anesthesia workshop on Thursday. Mason as well as some other inspirational anesthesiologists, see these video interviews posted by Dr. Allison Fernandez for the Women of Impact in Anesthesiology project. Michael Champeau!
With so many options for premium operating tables, you may find it challenging to select a surgical table for your hospital. However, the operating tables market is growing and will reach US $1,043.41 With this forecasted growth rate, you need to know how to quickly find the best surgical tables for your operating room (OR).
Post-Anesthesia Care Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operating room and continues until they are stable enough to recover at home or in a hospital room. Their role in maintaining the flow of operations cannot be overstated.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operating room supplies. The video is posted here. The required parts are an operating room anesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps.
To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). The scrubs are enclosed in a device not dissimilar to a soda machine, and you need your ID to operate it.
The main questions as to whether a hospital or an ambulatory surgery center can resume elective surgery as of May 2020 are: What is the incidence of COVID-19 in your geographic area? The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operating room.
When you think of the operating room (OR), what comes to mind? At my first hospital, I visited the nursing director regularly to see if there were any openings. If patient status changes, you may have to switch what you are doing – stepping in to help anesthesia, for example. An intense and stressful work environment?
Sixty-six percent of surgeries in the United States take place as an outpatient , and many of these surgeries are performed at freestanding facilities distant from hospitals. If the patient is unstable, a physician, usually an anesthesiologist, will need to accompany the patient and the EMTs to the hospital emergency room.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
For non-anesthesiologists, who will not undergo three years of anesthesia residency training to become DL experts, learning video laryngoscopy instead of direct laryngoscopy makes sense. Of course none of the anesthesiologists or operating room personnel are dishonest, but preventing theft of these small valuable devices would be difficult.
An anesthesia emergency occurs without warning. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group. Your patient’s vital signs are dropping.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The hospital was Watertown Regional Medical Center, located in Watertown, Wisconsin , population 23,861, midway between Milwaukee and Madison. In a word, no. See this link.
Anesthesia departments are crucial to the success of operating rooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Here are five warning signs that your anesthesia team might be underperforming: 1.
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists typically spend 90+% of their working hours in the operating room.
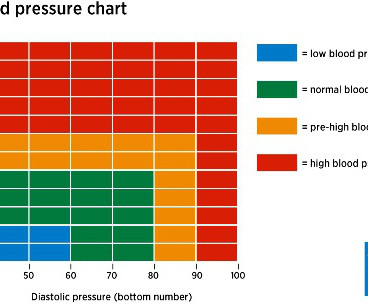
In the operating room, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
Or is it an expensive gadget for hospitals and surgeons to market and attract potential patients? Video laparoscopy surgical equipment and the longer operating times were increased expenses, but the advantages of outpatient surgery and quicker recovery made the new technique the standard of care for many surgeries within the abdomen.
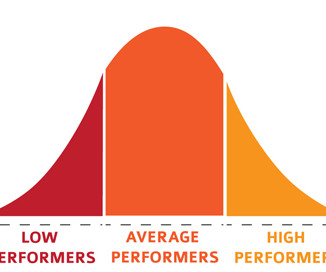
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% The patient does well, and is discharged from the PostAnesthesia Care Unit in excellent condition. The patient objects. You’re the greatest.”
CardioPulmonary Resuscitation in the Operating Room The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operating room. Both were published in the journal Anesthesia and Analgesia.
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. Do you think patients want a friendly anesthesiologist who is all thumbs in the operating room? No, they want a skilled practitioner.
If you wonder how much the anesthesia scene has changed significantly over the past four decades, check out this narrative: In 1986 I was in my second and final year of anesthesia residency training at Stanford, and I was looking for a job. I heard about an opening with a busy private practice anesthesia group in Southern California.
Trauma is the most common indication for surgery and anesthesia of an acutely intoxicated individual, but other types of surgical emergencies can result from drug misuse, including vascular dissection and hemorrhagic complications linked to certain stimulants. The CAGE questionnaire can be used to this end. References 1.
Primary Consultant Anesthesiologist The “Preoperative Evaluation” chapter in our Bible, Miller’s Anesthesia , is 80 pages long—one of the longest chapters in the book. It’s almost June, and hundreds of anesthesia residents are about to graduate from residency programs. Read on and I’ll explain why. His clinic resulted in 87.9%
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
Learn tips about establishing guiding principles and developing key committees in support of Leadership and Operational Management to initiate breakthrough performance. This session is valuable to hospital Perioperative Services Leaders (Executive Administrators, Directors, Nurse Managers), Anesthesia Providers, and C-Suite Executives.
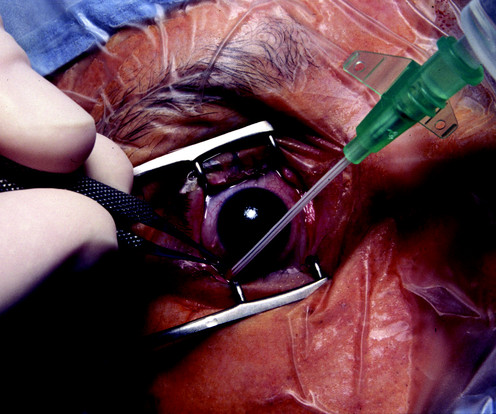
The boy suffers a penetrating open eye injury, and is taken to the nearest hospital. You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists.
Round up your smartest engineer buddies and invent the electronic medical recordkeeping system every hospital needs. Doctors and hospitals who failed to adopt a government-approved EMR system by the end of 2014 faced cutbacks in their Medicare reimbursements. hospitals have an EMR system. How can a hospital recoup this cost?
In this blog post, we’ll provide an insider’s perspective on a CRNA’s exciting and rewarding career by highlighting their daily responsibilities, how they overcome challenges, and their tremendous impact on patient care and the health field. To begin, it’s essential to understand the role of a CRNA.
The Merriam-Webster online dictionary defines private practice as: “a professional business (such as that of a lawyer or doctor) that is not controlled or paid for by the government or a larger company (such as a hospital).” A private practice anesthesia group needn’t be a physician-only group. Let’s look at the issues. It depends.
If you’re wondering how your hospital or surgery center could benefit from the integration of these professionals, here are three ways that they improve patient outcomes. Shorten surgery times According to the Canadian Journal of Surgery, operations involving skilled surgical assistants are completed 30 percent faster.
Anesthesia EMR software is a driving force behind this change, heralding an era that gives clinicians more time with the patient, and helps improve operations. Improvements in Data Collection Anesthesia EMR software isn’t just about documenting medical records electronically.
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Anesthesia personnel will be in great demand.
This article will delve into what PLIF entails, its benefits, the surgical procedure, and post-operative care, providing you with a comprehensive understanding of this critical spinal surgery. These may include infection, bleeding, nerve damage, and issues related to anesthesia. What is Posterior Lumbar Interbody Fusion (PLIF)?
The video provides answers to individuals who have obstructive sleep apnea and are contemplating surgery and anesthesia. Patients with OSA frequently present for surgery, and all anesthesia professionals must be aware of the risks involved with anesthetizing OSA patient. Risks of anesthesia and the OSA patient?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content