This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Perioperative hypothermia, defined as a core body temperature below 36°C, is a frequent and preventable complication associated with anesthesia and surgical procedures. The post-operative phase is crucial for reinforcing normothermia and supporting patient recovery, yet it is often overlooked in thermal management.
Surgeons severely dislike it when their cases are delayed, and delays negatively impact hospital financial performance. Getting Started Avoiding case delays starts with tracking the major causes and using AI to proactively identify patients and procedures with a high probability of not starting on time. Inclusion = ownership!
Last week, I encounter a patient that I’ve taken care of twice before (how likely is it amongst 30 CRNAs at the hospital that I get to take care of him 3 times in a row?). Last week, I encounter a patient that I’ve taken care of twice before (how likely is it amongst 30 CRNAs at the hospital that I get to take care of him 3 times in a row?).
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
This concept has gained traction in recent years, reflecting a broader understanding of the benefits of optimizing health before undergoing surgical procedures. By addressing these factors, prehabilitation aims to boost the patient’s resilience and functional capacity, enabling them to recover more swiftly and effectively post-surgery.
Ahead of a visit to the hospital for a surgical procedure, patients often have plenty of questions about what to expect — and can be plenty nervous. Personalized Experiences for Hospital Patients Patients can get overwhelmed with the amount of pre-operative information.
Though all APRNs undergo extensive training to achieve their advanced degree, each type obtains a different skillset, with CRNAs focused on anesthesia care. In contrast to other APRNs, CRNAs are specially trained to provide anesthesia to patients in settings such as hospitals, clinics, private practices, and doctors’ offices.
Modern tools designed for anesthesia documentation and billing accuracy can reduce missed charges and improve coding precision. By automating these processes, hospitals enhance revenue cycle management while freeing clinicians to focus more on patient care. Hospitals must find ways to maximize efficiency with fewer team members.
Lidocaine is an amide local anesthetic commonly used for local or topical anesthesia. Intravenous lidocaine also appeared to have advantageous effects [RJ1] on gastro-intestinal motility, length of hospital stays, postoperative nausea, and opioid consumption. Because of these benefits, Chu et al.
You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5%
The main questions as to whether a hospital or an ambulatory surgery center can resume elective surgery as of May 2020 are: What is the incidence of COVID-19 in your geographic area? When I’m at Stanford Hospital or the surgery centers in our area I’m confident the environment is safe. It depends.
Primary Consultant Anesthesiologist The “Preoperative Evaluation” chapter in our Bible, Miller’s Anesthesia , is 80 pages long—one of the longest chapters in the book. It’s almost June, and hundreds of anesthesia residents are about to graduate from residency programs. Read on and I’ll explain why. His clinic resulted in 87.9%
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? Should you buy these books, or should you advocate that your hospital purchase them for the medical library? All anesthesia providers should have access to the current two-volume 3112-page edition.
Sixty-six percent of surgeries in the United States take place as an outpatient , and many of these surgeries are performed at freestanding facilities distant from hospitals. If the patient is unstable, a physician, usually an anesthesiologist, will need to accompany the patient and the EMTs to the hospital emergency room.
Peripheral nerve blocks are a type of regional anesthesia that involve injecting local anesthetics and other painkillers near specific nerves or groups of nerves. These are also commonly used in orthopedic procedures. In comparison, intra-articular blocks involve injecting medications directly into the joint space.
Post-Anesthesia Care Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operating room and continues until they are stable enough to recover at home or in a hospital room. PACU nurses contribute significantly to this efficiency.
The video provides answers to individuals who have obstructive sleep apnea and are contemplating surgery and anesthesia. Patients with OSA frequently present for surgery, and all anesthesia professionals must be aware of the risks involved with anesthetizing OSA patient. Risks of anesthesia and the OSA patient?
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). What can we expect in the next 10 years of anesthesiology?
They play a crucial role in healthcare by ensuring patient safety and comfort before, during, and after surgical procedures. Anesthesia is a vital tool in modern medicine and CRNAs serve as experts in providing this medical service to patients. Proper planning creates the best possibility for surgical procedures to go well.
This article will delve into what PLIF entails, its benefits, the surgical procedure, and post-operative care, providing you with a comprehensive understanding of this critical spinal surgery. The procedure involves accessing the spine from the back (posterior) to remove the damaged disc and fuse the adjacent vertebrae together.
Anesthesia departments are crucial to the success of operating rooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Here are five warning signs that your anesthesia team might be underperforming: 1.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
Or is it an expensive gadget for hospitals and surgeons to market and attract potential patients? Anesthesia for laparoscopy was similar to the anesthetic for open abdominal surgery. Almost every anesthesiologist in America has experience with surgery using the da Vinci robot system.
18, 2024 While Hospital Outpatient Department (HOPD) Ambulatory Surgery Centers receive higher reimbursement rates than freestanding Ambulatory Surgery Centers ( ASCs ), hospital systems are increasingly interested in transitioning their freestanding HOPDs to ASCs. Updated Sept. Let’s dive right in! Absolutely not!
Dermatologists perform procedures with their hands, including biopsies or the resection of lesions. But one large subset of anesthesia work closely mimics the lifestyle of dermatology practice. These procedures are low-risk surgeries which don’t disturb a patient’s physiology in any significant way.
Posterior cervical fusion is a surgical procedure designed to address various conditions affecting the cervical spine. This procedure is essential for patients suffering from severe neck pain, instability, or spinal deformities. What is Posterior Cervical Fusion?
Round up your smartest engineer buddies and invent the electronic medical recordkeeping system every hospital needs. Round up your smartest engineer buddies and invent the electronic medical recordkeeping system every hospital needs. hospitals have an EMR system. Stanford Hospital adopted EPIC over ten years ago.
Placing a catheter into the tiny radial artery in a child’s wrist is one of the most difficult procedures in our specialty. Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. binocular Moverio BT-35E smart glasses A South Korean group led by Dr. Y.E.
You’ve probably heard about the game-changing benefits of implementing an Anesthesia Information Management System (AIMS): time savings; ease of use; greater legibility and accuracy; reliability and defensibility; improved patient monitoring, and giving clinicians more time to focus on the patient. This will improve efficiency.
Preparation for ALIF Surgery The ALIF Surgery Procedure Recovery and Rehabilitation Frequently Asked Questions SpecialtyCare’s ALIF Surgery Services 1. Introduction to ALIF Surgery Anterior Lumbar Interbody Fusion (ALIF) surgery is a type of spinal fusion procedure designed to alleviate pain and improve stability in the lower back.
To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Your hospital contains multiple operating rooms, and today you are in room #10.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operating rooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
Trauma is the most common indication for surgery and anesthesia of an acutely intoxicated individual, but other types of surgical emergencies can result from drug misuse, including vascular dissection and hemorrhagic complications linked to certain stimulants. The CAGE questionnaire can be used to this end.
In the operating room, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
What’s the relationship between alcohol and anesthesia? Miller’s Anesthesia , 9 th edition, Chapter 31, Preoperative Evaluation) All adults and adolescents should be questioned regarding their history of alcohol use prior to anesthesia. Is this OK? The intersection of an alcohol-addicted patient and surgery is therefore common.
According to an American Hospital Association (AHA) survey of community hospitals, nearly 50% of responding hospitals reported at least 21 drug shortages within the first 6 months of 2011, and more than 99% of hospitals reported at least 1 drug shortage within the same time period. min vs. 6.0 ± 2.1 min,
If you’re wondering how your hospital or surgery center could benefit from the integration of these professionals, here are three ways that they improve patient outcomes. Allow more procedures to be performed When surgery times are shortened, surgeons and other surgery providers are able to work with more patients per day.
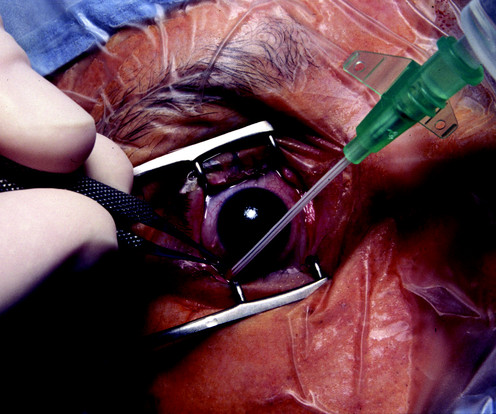
The boy suffers a penetrating open eye injury, and is taken to the nearest hospital. You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists.
A recent 2024 publication in JAMA looked at 8429 surgical procedures from March 2021 to December 2022 in a single institution. The anesthesiologist could indirectly visualize the patient’s vocal cords, which enabled the placement of the endotracheal tube into the windpipe. I utilize VL for difficult airway cases or emergency cases.
Dr. Gawande is a Professor of Surgery at Harvard/ Brigham and Women’s Hospital, and is the bestselling author of multiple nonfiction books directed at healthcare topics. This proposed elimination of wasteful spending would decrease the demand for anesthesia professionals. Pearl writes, “ It’s estimated that 25 percent of all U.S.
How soon will we see robotic anesthesia in our hospitals and surgery centers? Most of these discoveries originated in Silicon Valley, just miles outside Stanford University Hospital where I’ve been working for the past 42 years. Our medical world inside the hospital has changed more slowly. Relatively little.
Yet, with a single minute in the OR costing as much as $120, ASCs, hospital outpatient departments (HOPD), and ORs regularly waste much more than that. The reasons for low OR utilization rates are multifactorial, yet they often trace back to ineffective pre-anesthesia testing processes. Take $120 and put it in the garbage. Do it again.
You’re in the middle of your medical school years, and wondering what specialty to pursue. There are two major forks in the road when trying to choose the career that suits your emotional make-up and work ethic. The sooner you understand these two forks in the road, the better off you’ll be. CLINIC DOCTOR OR ACUTE CARE DOCTOR?
Anesthesia EMR software is a driving force behind this change, heralding an era that gives clinicians more time with the patient, and helps improve operations. Improvements in Data Collection Anesthesia EMR software isn’t just about documenting medical records electronically. Its most significant contribution is the gift of time.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content