This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This is a futuristic technology, and its use may connote that the hospital or surgery center is at the cutting edge of monitoring and safety equipment (despite the lack of any data to confirm this advantage at this time). Would the addition of smart glasses for routine monitoring be an overdose of technology in the operatingroom cockpit?
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. Imagine this: It’s the year 2034.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. You complete your morning bathroom and breakfast routines, and leave your residence at 0630 hours for the hospital. You take the elevator to the third floor and proceed to the locker room.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
Dental cases are common, and are frequently referred to a hospital because the typical care systems at an outpatient surgery center or a dental office are inadequate to complete a successful anesthetic. The most common anesthesia induction technique in children and toddlers is an inhalation induction with sevoflurane.
You’re a Medical Director or medical educator, and you’re scheduled to deliver a lecture on the management of two or three common operatingroom emergencies. You’re an expert witness or a member of your hospital’s Quality Improvement committee, charged with reviewing the unfortunate outcome of an operatingroom medical complication.
The main questions as to whether a hospital or an ambulatory surgery center can resume elective surgery as of May 2020 are: What is the incidence of COVID-19 in your geographic area? The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom.
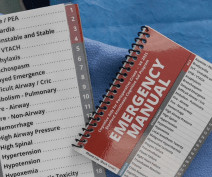
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. Why Did Take Me So Long To Wake From GeneralAnesthesia?
Consider this: if a hospital purchased 20 McGrath scopes at $3899, with the small pocket size of a McGrath scope it would only be a matter of time before some of the scopes would disappear. The university hospital where I work owns multiple GlideScopes and C-MAC video scopes but stops far short of one for every room.
Anesthesiologists typically spend 90+% of their working hours in the operatingroom. A busy surgeon will spend 50% of their time in the operatingroom, and the other 50% in preoperative clinic, postoperative clinic, or rounding on patients in the hospital. Why Did Take Me So Long To Wake From GeneralAnesthesia?
I contacted the group via telephone, mailed them my resume, and they invited me to travel to their hospital for an interview. When I arrived at their hospital, I donned scrubs and was ushered from operatingroom to operatingroom to meet 15 or 20 attending anesthesiologists while they worked. I was excited.
Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. Plan: cleared for generalanesthesia providing ECG and labs are normal. Why Did Take Me So Long To Wake From GeneralAnesthesia? What Are the Common Anesthesia Medications?
No one wants a partner who repeatedly creates conflict in the workplace, who initiates conflict with a surgeon in the operatingroom, a nurse in the post anesthesia care unit, or an administrator. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom?
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The hospital was Watertown Regional Medical Center, located in Watertown, Wisconsin , population 23,861, midway between Milwaukee and Madison. A doctor or a nurse?
Sixty-six percent of surgeries in the United States take place as an outpatient , and many of these surgeries are performed at freestanding facilities distant from hospitals. If the patient is unstable, a physician, usually an anesthesiologist, will need to accompany the patient and the EMTs to the hospital emergency room.
Anesthesiologists still work in hospitaloperatingrooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
Some were academic professors, some were trainees at a university, and some were community anesthesiologists either in my group or in other anesthesia companies. We’re entering an era of metrics for physicians, in which the government and hospital systems will collect data to monitor quality and performance. Stick up for yourself.
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? Should you buy these books, or should you advocate that your hospital purchase them for the medical library? Why Did Take Me So Long To Wake From GeneralAnesthesia?
In the operatingroom, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. What Are the Common Anesthesia Medications?
If you’re wondering how your hospital or surgery center could benefit from the integration of these professionals, here are three ways that they improve patient outcomes. Shorten surgery times According to the Canadian Journal of Surgery, operations involving skilled surgical assistants are completed 30 percent faster.
New York, NY – The era of COVID-19 has pushed the envelope in hospitals across the world, challenging care delivery models and allowing one ventilator to ventilate 600 patients at once. Shortly after, the spinal anesthetic wore off and the patient was quickly placed under generalanesthesia.
Or is it an expensive gadget for hospitals and surgeons to market and attract potential patients? The da Vinci surgeon sits at a console in the corner of the operatingroom, with his back to the patient and his face in a 3-D viewer, which gives a high-definition, magnified view of the surgical site.
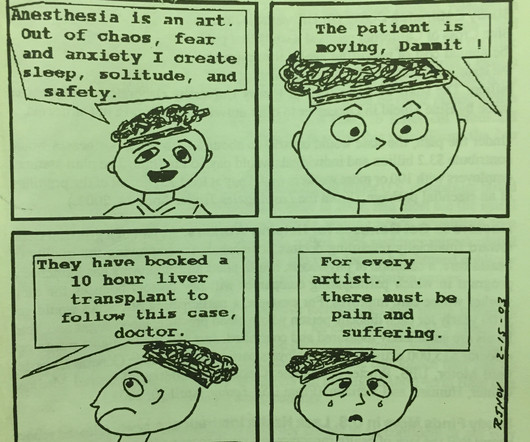
Baker is doing in panel 4, but the anesthesiologist’s rapid heart rate and the adrenaline rush in high pressure operatingroom situations accompany the growth of every anesthesiologist from inexperience trainee to seasoned professional. Why Did Take Me So Long To Wake From GeneralAnesthesia?
The Merriam-Webster online dictionary defines private practice as: “a professional business (such as that of a lawyer or doctor) that is not controlled or paid for by the government or a larger company (such as a hospital).” A private practice anesthesia group needn’t be a physician-only group. Let’s look at the issues.
I agree with him that the current cumbersome EHRs come between doctors and patients during hospital care. My criticisms include: Different EHRs at different hospitals are unable to communicate with each other. If you work at different hospitals with different EHRs, you have to be trained and retrained in multiple EHR platforms.
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Why Did Take Me So Long To Wake From GeneralAnesthesia?
Round up your smartest engineer buddies and invent the electronic medical recordkeeping system every hospital needs. Doctors and hospitals who failed to adopt a government-approved EMR system by the end of 2014 faced cutbacks in their Medicare reimbursements. hospitals have an EMR system. How can a hospital recoup this cost?
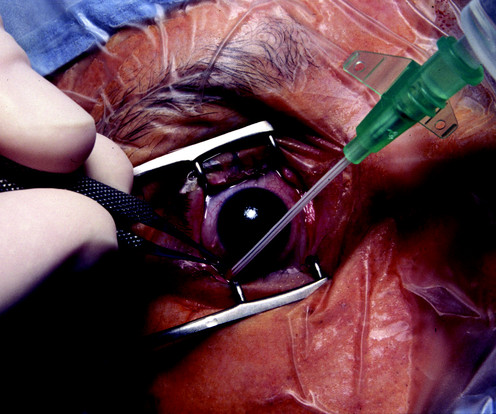
The boy suffers a penetrating open eye injury, and is taken to the nearest hospital. You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists.
In 2016 there were more than 224,000 operatingrooms in the United States , so tens of thousands of devices could be needed. Several large hospital systems, including the University of Arizona, Duke, University of North Carolina, and the Medical College of Wisconsin have purchased the devices for their operatingrooms.
At that age you’ll have a negative net worth, and you’ll be financially years behind your friends who went to work immediately out of college You’ll work long hours, including sleeping overnight in hospitals during your training. Answering phone calls or being summoned into the hospital at 3 a.m. 80-hour work weeks are common.
How can it be that generalanesthesia has ceased to evolve? Anesthesia in 2018 is markedly different from anesthesia in the 1990s. Most of the drugs in use haven’t changed, but current-day anesthesia providers practice in a cockpit surrounded by computers. Why Did Take Me So Long To Wake From GeneralAnesthesia?
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% It can happen, and it’s not that difficult in some hospital systems.
Dr. Gawande is a Professor of Surgery at Harvard/ Brigham and Women’s Hospital, and is the bestselling author of multiple nonfiction books directed at healthcare topics. From the exam room to the operatingroom, doctors today follow a clear set of protocols that Dr. Gawande helped establish.
Imagine you’re two months out of anesthesia training, working at a community hospital, and at 2 a.m. you need to induce emergency anesthesia for a 300-pound man who just ate a full meal of pizza and beer two hours earlier. You’re working alone without that anesthesia attending who stood next to you during residency training.
Even if a liberal Democrat wins the presidency and Congress gains a majority of Democrats in both the Senate and the House, they will all have to overcome multiple powerful lobbies, including the medical insurance industry, hospitals, the pharmacology industry, and organized physician groups. Risk during an anesthesia career is omnipresent.
Most medical careers require more than 50 hours a week, with time spent seeing patients in clinics or hospitals, charting on electronic medical records, and researching medical information from the internet or online libraries. Rick: The reason for Sam’s downfall from mainstream anesthesia is held out as a secret until the trial.
An operatingroomanesthesia practice is somewhat akin to being a taxi cab driver. The Veterans Affairs hospitals are currently pondering a move to allow CRNAs to practice independently without any physician anesthesiologist present. University anesthesia groups. National anesthesia companies.
Pursue a career as an acute care doctor if you prefer adrenaline-charged arenas such as the operatingroom, the intensive care unit, the labor and delivery suite, or the emergency room. Community physicians are individuals who work at your local clinic, your local hospital, or your local health maintenance organization.
Who is the Captain of the Ship in the operatingroom, the surgeon or the anesthesiologist? The Captain of the Ship doctrine was a 20 th century legal doctrine which held that, in an operatingroom, the surgeon was “liable for all actions conducted in the course of the operation.”
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following generalanesthesia. Will a shot of IV espresso be the stimulus for you to return to consciousness after your general anesthetic? I tried it on several of my patients who had prolonged awakening after generalanesthesia.
In a video featuring Spiro CEO Dimitri Sokolov , he quotes the number of expected and unexpected difficult intubations as 6 million per year in American operatingrooms, emergency rooms, and intensive care units. Each difficult intubation currently costs a hospital more than $14,000.
America’s hospitals are in fiscal chaos. Anesthesiologists work in hospitals, and when a hospital closes, anesthesiologists lose their jobs. Hospitals are losing money, particularly when it comes to the treatment of Medicaid/Medicare patients. 2 An anesthesia group’s success is closely tied to the fate of their hospital.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient. Love it or hate it, the EMR is here to stay.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content