This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transitioning from working as an ICU nurse to becoming a Certified Registered Nurse Anesthetist (CRNA) is a journey marked by immense growth but also profound challenges. Here’s a closer look at what this transition entails and how the Society of Future Nurse Anesthetists (SFNA) supports aspiring CRNAs in navigating these changes.
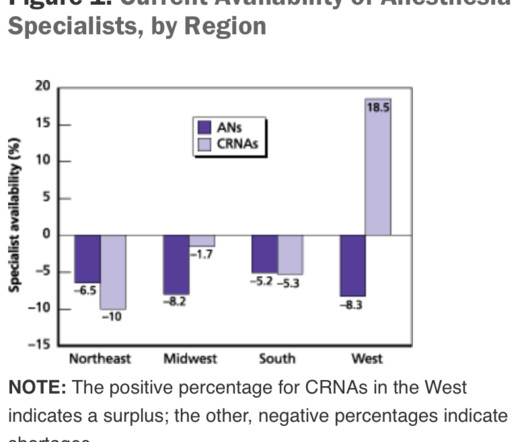
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
In this blog post, we’ll provide an insider’s perspective on a CRNA’s exciting and rewarding career by highlighting their daily responsibilities, how they overcome challenges, and their tremendous impact on patient care and the health field. To begin, it’s essential to understand the role of a CRNA.
Without a doubt, the operatingroom (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. to improve the bottom line, changes to the existing anesthesia staffing model may help. link] The Three Anesthesia Staffing Models: The optimal hospital staffing model should: 1.
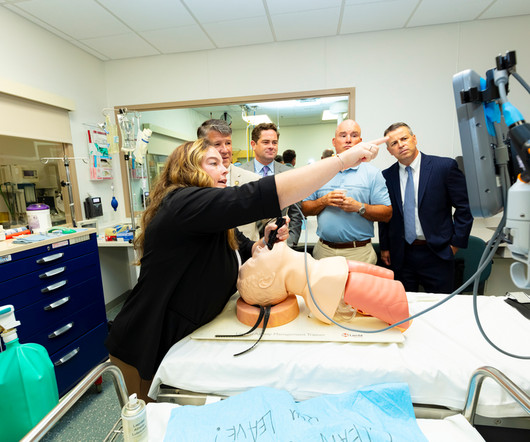
Seeing is believing and several northeastern Pennsylvania lawmakers and staff got a firsthand look at just a few of the intensive education and training programs that students must master to become certified registered nurse anesthetists (CRNAs). Eddie Day Pashinski (D-Luzerne) to visit and check out the university’s simulation labs.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). (He In a word, no. No, they are not.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10.
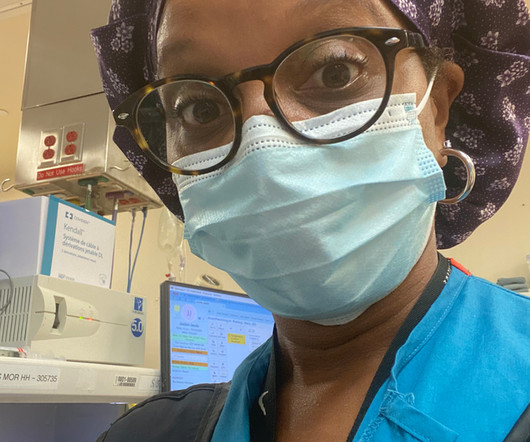
Advanced Practice Provider Spotlight: Certified registered nurse anesthetist shares perspective on caring for diverse patients Posted April 11, 2023 by ,Penn State Health News Prolung Ngin , a certified registered nurse anesthetist (CRNA) at Penn State Health Milton S.
The only way to end the sedative effects of propofol is for an anesthesia professional to support the airway, breathing, and circulation of the patient until the drug effects of propofol wear off in time. I’ve never administered a dose of flumazenil in my entire career, nor have most of my anesthesia colleagues.
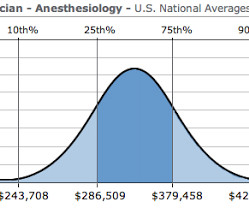
Let me begin by offering two anecdotes: I was an invited visiting anesthesia professor at a major university this year, and following one of my lectures an anesthesiology resident approached me for a discussion. The demand for anesthesia services will grow. How much money does an anesthesiologist earn? It depends.
Anesthesiologists still work in hospital operatingrooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. Careers in anesthesia are intellectually stimulating, emotionally gratifying, and have high median salaries and ultra-low unemployment.
Dawn Bent, DNP, MSN, CRNA , didn’t choose to be a nurse anesthetist as much as the profession chose her. She didn’t know what that was, and so he took her over to the operatingroom and let her see the profession in action. “The We were all students at one point.”
Who is the Captain of the Ship in the operatingroom, the surgeon or the anesthesiologist? The Captain of the Ship doctrine was a 20 th century legal doctrine which held that, in an operatingroom, the surgeon was “liable for all actions conducted in the course of the operation.”
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. INTRAOPERATIVE DECISION A 60-year-old man with a history of hypertension is having a knee arthroscopy surgery under general anesthesia. This could indicate a cardiac event or a complication related to the anesthesia.
Anesthesia is a hands-on specialty. Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Since the development of the internet, anesthesia practice has changed forever.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. The patient consents.
Every anesthesia provider must learn to free-solo anesthesia early in his or her career. A typical hospital will have dozens of other anesthesia providers working in the same building. Commercial aviation is sometimes compared to anesthesia practice. In anesthesia there is no guaranteed second anesthesiologist.
He writes, “Our specialty, anesthesia, has suffered an identity crisis for decades. In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operatingroom. Read my column on bullying in the operatingroom. Hold your heads high.
This is what the anesthesia experience is like for most patients: You show up for surgery, and some anesthesia professional you’ve never met or talked to appears 10 minutes before you are to be wheeled into the operatingroom. The anesthesia professional might be an MD, a CRNA, or both a MD and a CRNA might be involved.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of general anesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). If the patient has an ET tube, it is usually removed.
Very few patients die in the operatingroom, but significant numbers die in the weeks that follow. At times, physician anesthesiologists employ certified registered nurse anesthetists (CRNAs) to assist them in what is called the anesthesia care team (ACT) model. Are CRNAs and anesthesiologists equals?
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
by PennLive.com Patients undergoing surgery or procedures requiring anesthesia are safe when cared for by a physician anesthesiologist, a certified registered nurse anesthetist (CRNA), or both. 3) relates to outdated and restrictive laws that prevent CRNAs from practicing to their fullest scope. Published: Jan.
I’d already secured my medical staff privileges and my appointment to the anesthesia service. I entered the hallway of the operatingroom complex. Hibbing General had only six operatingrooms, compared to the 40 rooms at Stanford. The operatingroom was small, a compact 30 feet by 30 feet.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content