This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The operatingroom is a fast-paced, high-stakes environment where precision, teamwork, and vigilance are non-negotiable. Safe surgical care demands seamless collaboration between surgeons, nurses, techs, and anesthesia providers, so that we can achieve excellent outcomes. 4 But what about operatingroom nurses specifically?
Of course, my background includes being a surgical technician and PACU (postoperative care unit) nurse so finding a CRNA to shadow was pretty easy. But I personally chose to shadow a CRNA for 40 hours total even though I worked in the operatingroom prior. And many operatingrooms have a no cell phone policy anyway.
Who is the Captain of the Ship in the operatingroom, the surgeon or the anesthesiologist? The Captain of the Ship doctrine was a 20 th century legal doctrine which held that, in an operatingroom, the surgeon was “liable for all actions conducted in the course of the operation.”
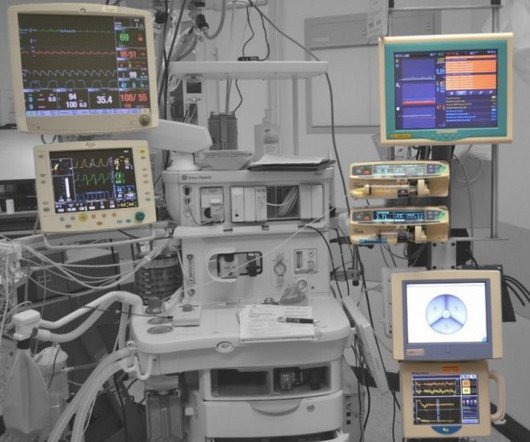
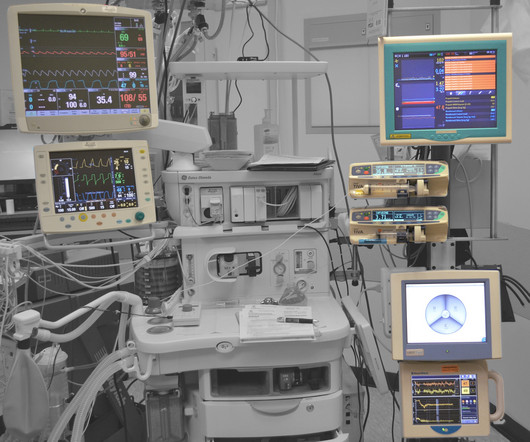
Anesthesiologists watch vital sign monitors continuously in the operatingroom every day, and have more experience following vital sign abnormalities minute-to-minute than other physicians. The blood oxygen level, or oxygen saturation level, is equivalent to what a pulse oximeter measures in the operatingroom.
Picis is known for its reliable, intuitive software that helps hospitals improve operatingroom efficiency (OR), enhance staff communication and coordination, reduce scheduling delays and conflicts, and optimize surgical workflow and patient flow.
It’s a path that demands not only clinical excellence but also a significant shift in roles—from direct patient care in a high-intensity setting to the precision and autonomy of anesthesia. Understanding the Shift The transition from ICU to operatingroom (OR) involves a fundamental change in responsibilities.
OperatingRoom (OR) nurses, also known as perioperative nurses, play an essential role in surgeries. OR nurses are the backbone of the operatingroom, advocating for patients and supporting the entire surgical team. The post What is an OR Nurse and What Do They Do in the OperatingRoom?
Many factors affect the operatingroom (OR) and surgery success, ranging from patient-related factors to resource-related factors to even clinician-related factors. In the operatingroom (OR), teamwork is crucial for ensuring patient safety. The American Journal of Surgery, vol. 1] Arora et al. Arora et al.
Anesthesiology residents play an important role in the operatingroom (OR), assisting with patient care while also undergoing rigorous training to become skilled anesthesiologists. Their responsibilities encompass a range of tasks, from preoperative evaluations to the administration of anesthesia and postoperative care.
including pediatric open heart surgery, and pediatric surgery involving major blood loss). This is a futuristic technology, and its use may connote that the hospital or surgery center is at the cutting edge of monitoring and safety equipment (despite the lack of any data to confirm this advantage at this time).
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists. million charts were studied.
If you were consolidating five disparate sites of care into a new 12-OR surgery center, what would you do to set it up for success? Luke’s wanted the surgery center to run with the operational mentality of an ambulatory surgery center (ASC). Through their work, they helped St. Crucially, Sullivan helped the St.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
In recent years, engineers have developed closed-loop AI machines that can administer appropriate doses of anesthetics without human input , as described in The Washington Post article, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Thus, we might ask, ‘What happens to the operator/clinician involved?’
When you think of the operatingroom (OR), what comes to mind? When a patient is in surgery, they need an advocate as they are unable to advocate for themselves. Managing the room, including supplies, equipment, lighting and documentation. Eye surgery is an example of a surgery that may take less than 30 minutes.
Post-Anesthesia Care Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operatingroom and continues until they are stable enough to recover at home or in a hospital room. PACU nurses contribute significantly to this efficiency.
Cardiovascular surgery is one of the most complex and high-stakes fields in medicine. Their role is crucial for ensuring a smooth operation, but what exactly do they do, and why are they so essential in cardiovascular surgeries? What is a Surgical Assistant’s Role in Cardiovascular Surgery?
An important question for many Americans is, “Is it safe for me to have surgery during this COVID pandemic?” The main questions as to whether a hospital or an ambulatory surgery center can resume elective surgery as of May 2020 are: What is the incidence of COVID-19 in your geographic area? It depends.
Almost every anesthesiologist in America has experience with surgery using the da Vinci robot system. Is robot surgery a miraculous futuristic device that advances surgery to a higher plain? Until the 1990s most abdominal surgery was done through an open incision. To answer these questions let’s first review some history.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10.
There are Two Laws of Anesthesia, according to surgeon lore. The patient must wake up (when the surgery is over). Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs.
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. Both were published in the journal Anesthesia and Analgesia.
Open abdominal surgeries became laparoscopies, with the surgeon focused on a two-dimensional video screen while he or she manipulated instruments inside the abdomen. McGrath Video Laryngoscope Limitations of video laryngoscopy include: The price of purchasing one GlideScope for our multispecialty ambulatory surgery center was $14,000.
An anesthesia emergency occurs without warning. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group. Your patient’s vital signs are dropping.
The February 2020 edition of Anesthesiology , our specialty’s preeminent journal, published an article on robotic anesthesia. 1 The accompanying editorial by Dr. Thomas Hemmerling was titled “Robots Will Perform Anesthesia in the Near Future. ” robotic) anesthesia is at least as good as the best human anesthesia.
In the highly specialized field of plastic surgery, having a reliable and skilled team is essential to delivering top-notch results and ensuring patient safety. Their responsibilities include: Preoperative Preparation: Ensuring the operatingroom is ready, sterilizing instruments, and preparing patients for surgery.
Many patients require preoperative clearance prior to surgery, especially patients with significant medical problems or at extremes of age. Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. Let’s choose an illustrative example.
In the operatingroom, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). (He In a word, no. No, they are not.
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? Digital access to all this written expertise can be at your fingertips anywhere, including in the operatingroom suite. ebook $165.29, hardcover $126.17) The Stanford Emergency Manual.
The new device being discussed is the iControl-RP anesthesia robot. THE iCONTROL-RP ANESTHESIA ROBOT On May 15, 2015, the Washington Post published a story titled, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” A score of 40 – 60 is considered an optimal amount of anesthesia depth.
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
In this blog post, we’ll provide an insider’s perspective on a CRNA’s exciting and rewarding career by highlighting their daily responsibilities, how they overcome challenges, and their tremendous impact on patient care and the health field. CRNAs received specialized training that is critical in surgeries and healthcare.
3 Ways Surgical Providers Improve Patient Outcomes Surgical providers—surgical assistants, nurses, and surgical technologists—provide aid during surgery to doctors. They assist in exposure, closure, hemostasis, and other intraoperative technical functions that ultimately ensure the surgery is successful.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia.
If you wonder how much the anesthesia scene has changed significantly over the past four decades, check out this narrative: In 1986 I was in my second and final year of anesthesia residency training at Stanford, and I was looking for a job. I heard about an opening with a busy private practice anesthesia group in Southern California.
If your portfolio is looking for an acquisition positioned to leverage emerging trends in healthcare and deliver sustainable growth, investing in an Ambulatory Surgery Center (ASC) could be the perfect fit. With rising anesthesia costs and stagnating reimbursements, ASCs’ margins are thinner than they were even five years ago.
Photo by Magali Gauthier/The Almanac Between his time in the operatingroom, teaching, and raising his three sons, Atherton resident Dr. Rick Novak has found time to write two novels. The post DOCTOR BY DAY, SCI-FI WRITER BY NIGHT appeared first on The anesthesia consultant.
Is your doctor an experienced anesthesia provider or a newbie? The list below chronicles the crescendo of growth of as I’ve witnessed it from a newly-trained anesthesia doctor to an expert practitioner. In my view, inexperienced anesthesia providers are more likely to: Be nervous/anxious. This observation is no surprise.
Sixty-six percent of surgeries in the United States take place as an outpatient , and many of these surgeries are performed at freestanding facilities distant from hospitals. Her breathing tube had been removed, but she developed upper airway obstruction in the PostAnesthesia Care Unit (PACU) and needed urgent reintubation.
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
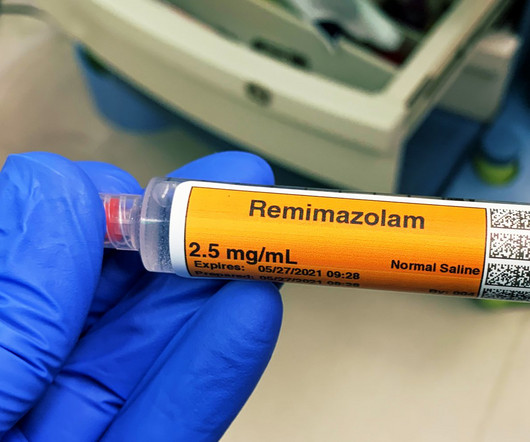
The only way to end the sedative effects of propofol is for an anesthesia professional to support the airway, breathing, and circulation of the patient until the drug effects of propofol wear off in time. I’ve never administered a dose of flumazenil in my entire career, nor have most of my anesthesia colleagues.
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom? Why Did Take Me So Long To Wake From General Anesthesia?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content