This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The operatingroom is a fast-paced, high-stakes environment where precision, teamwork, and vigilance are non-negotiable. Safe surgical care demands seamless collaboration between surgeons, nurses, techs, and anesthesia providers, so that we can achieve excellent outcomes. So How Do We Prevent Nurse Burnout?
Of course, my background includes being a surgical technician and PACU (postoperative care unit) nurse so finding a CRNA to shadow was pretty easy. But I personally chose to shadow a CRNA for 40 hours total even though I worked in the operatingroom prior. Turn off your cell phone. This is just common courtesy.
Who is the Captain of the Ship in the operatingroom, the surgeon or the anesthesiologist? The Captain of the Ship doctrine was a 20 th century legal doctrine which held that, in an operatingroom, the surgeon was “liable for all actions conducted in the course of the operation.”
Transitioning from working as an ICU nurse to becoming a Certified Registered Nurse Anesthetist (CRNA) is a journey marked by immense growth but also profound challenges. Here’s a closer look at what this transition entails and how the Society of Future Nurse Anesthetists (SFNA) supports aspiring CRNAs in navigating these changes.
OperatingRoom (OR) nurses, also known as perioperative nurses, play an essential role in surgeries. OR nurses are the backbone of the operatingroom, advocating for patients and supporting the entire surgical team. What Does an OR Nurse Do?
Happy CRNA Week 2024 A lot has happened The last two months I moved to San Diego Oh what joyous fun A lot of changes for my family and for me New preschool, grandparent help, New workplace A lot of things to learn “Reprogramming” I’d like to say Each NORA (Non-OperatingRoomAnesthesia) location Different than the next A lot of new people More than (..)
When you think of the operatingroom (OR), what comes to mind? I spent more than 40 years working in nursing before joining 3M five years ago. At my first hospital, I visited the nursing director regularly to see if there were any openings. Managing the room, including supplies, equipment, lighting and documentation.
Anesthesia vital signs monitor display A second and more compelling use for smart glasses would be the display of a patient’s vital sign monitoring in real time on the smart glass screen, so that an anesthesiologist is in constant contact with the images of the vital sign electronic monitors. Let me give you a historical perspective.
Many factors affect the operatingroom (OR) and surgery success, ranging from patient-related factors to resource-related factors to even clinician-related factors. In the operatingroom (OR), teamwork is crucial for ensuring patient safety. Journal of PeriAnesthesia Nursing, Oct. 24–30, [link] 2.
In the surgery center specifically, Sullivan’s team helped establish an operatingroom committee. Something as simple as changing blocks will affect what rooms will run cases, what different staff segments need to prepare, and what’s available for add-ons. The crux of the issue sat with the incumbent all-nurse staffing model.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
Post-Anesthesia Care Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operatingroom and continues until they are stable enough to recover at home or in a hospital room. PACU nurses contribute significantly to this efficiency.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operatingroom supplies. The video is posted here. The required parts are an operatingroomanesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps.
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. Both were published in the journal Anesthesia and Analgesia.
As a registered nurse, you would think that all this technology supporting the hiring process of nurses would lead to improvements or faster response times but if you have ever spent time on a single application website then you know the frustration and effort that simply goes to waste. What a disaster?!
A doctor or a nurse? On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “
Certified Registered Nurse Anesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. Anesthesia is a vital tool in modern medicine and CRNAs serve as experts in providing this medical service to patients. To begin, it’s essential to understand the role of a CRNA.
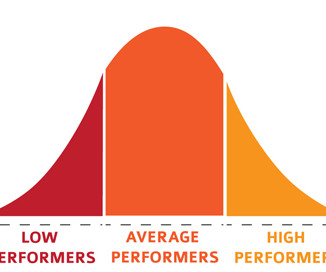
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). It’s also not uncommon for the patient to be breathing room air during transport.
When you enter the healthcare facility, a nurse will question you regarding virus symptoms, and will screen you by taking your temperature. The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom.
Anesthesia departments are crucial to the success of operatingrooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Here are five warning signs that your anesthesia team might be underperforming: 1.
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists typically spend 90+% of their working hours in the operatingroom.
Anesthesiologists still work in hospital operatingrooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. The job of a certified nurse anesthetist was listed as #11 on the Best Paying Jobs list. What Are the Common Anesthesia Medications?
Advanced Practice Provider Spotlight: Certified registered nurse anesthetist shares perspective on caring for diverse patients Posted April 11, 2023 by ,Penn State Health News Prolung Ngin , a certified registered nurse anesthetist (CRNA) at Penn State Health Milton S.
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom? No, they want a skilled practitioner.
3 Ways Surgical Providers Improve Patient Outcomes Surgical providers—surgical assistants, nurses, and surgical technologists—provide aid during surgery to doctors. Minimize patient time under anesthesia General anesthesia induces a sleep-like state using a combination of intravenous medications and inhaled gasses.
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% The patient does well, and is discharged from the PostAnesthesia Care Unit in excellent condition. He’s right. What happened?
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
Video laparoscopy surgical equipment and the longer operating times were increased expenses, but the advantages of outpatient surgery and quicker recovery made the new technique the standard of care for many surgeries within the abdomen. Anesthesia for laparoscopy was similar to the anesthetic for open abdominal surgery.
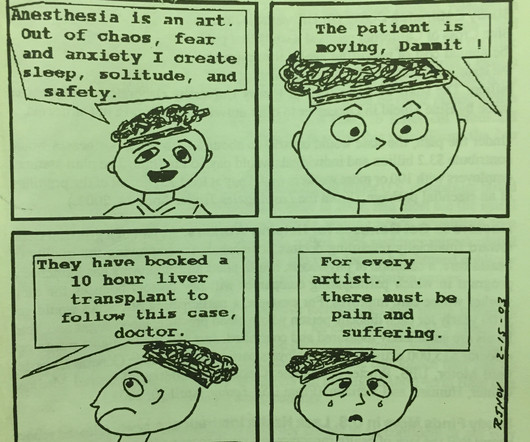
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From General Anesthesia?
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. Nurses consistently have their backs to patients as they type, type, type data into computer terminals.
Is the practice of anesthesia an art or a science? My career has bridged clinics, operatingrooms, intensive care units, emergency rooms, and helicopter trauma medicine. In the 21 st century operatingroom practice of anesthesiology, we typically have ten minutes to talk to a patient prior to rendering them unconscious.
The only way to end the sedative effects of propofol is for an anesthesia professional to support the airway, breathing, and circulation of the patient until the drug effects of propofol wear off in time. I’ve never administered a dose of flumazenil in my entire career, nor have most of my anesthesia colleagues.
You’ll become rich, and America’s doctors, nurses, and patients will bow to your achievement. Alas, doctors and nurses serve as data-entry technicians for the EPIC system of billing. EPIC is a poor system for doctors and nurses working in a hospital. If you’re a rising software engineer looking for a Holy Grail, this is it.
More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. Anesthesia personnel will be in great demand.
Having properly certified assistants at surgery usually makes the operation go faster, safer and smoothly. Having expert assistance can translate into shortening the time needed for anesthesia, increasing the safety of the procedure, reducing the surgical complication rates, and thus decreasing operatingroom costs.
During my anesthesia training at Stanford in the 1980s I was present through the growth years of Interplast, when traveling teams were dispatched to countries around the world to perform reconstructive surgeries on cleft lip and palate patients. Each Interplast anesthesia team included one faculty member and one or more resident.
Point/Counterpoint: How new is modern anesthesia? Are modern anesthesia techniques radically different from the methods of twenty years ago? How can it be that general anesthesia has ceased to evolve? What about regional anesthesia? Anesthesia in 2018 is markedly different from anesthesia in the 1990s.
Today I’m forwarding excellent information from a post by American viral specialist, James Robb MD , Fellow of the College of American Pathologists, a former Professor of Pathology at the University of California San Diego, and one of the first molecular virologists in the world to work on coronaviruses in the 1970s. I don’t think so.
My aim is to inform my readers, both anesthesia professionals and laypersons, that if Medicare for All becomes reality, there will be a dire consequence regarding anesthesia staffing and services to patients. What happens if every anesthesia patient pays only Medicare rates in a Medicare for All future? 75 X $76) + (.25
When a patient decompensates emergently at a freestanding ambulatory surgery center or in an operatingroom at a doctor’s office, the facility will call for an ambulance staffed with EMT personnel. Pulmonary edema fluid filled her lungs and filled the hoses of the anesthesia machine.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content