This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Rural hospital closures in the United States have become an increasingly concerning trend in recent years, with significant implications for healthcare access and quality in affected communities. Since 2010, over 130 rural hospitals have shut their doors, with a record 19 closures occurring in 2020 alone.
This week, we delve into financial planning for nurse anesthesia education, offering valuable tips on scholarships, grants, and budget management to help you achieve your goals without unnecessary financial strain. The post The Financial Path: Funding Your CRNA Education first appeared on The CRNA Chase.
Last week, I encounter a patient that I’ve taken care of twice before (how likely is it amongst 30 CRNAs at the hospital that I get to take care of him 3 times in a row?). Since I remembered how it took much longer from him to recover from anesthesia, I adjusted my anesthetic and he recovered much more quickly.
Today I’m posting a link to a video from an Italian hospital COVID-19 ward. The post VIDEO FROM AN ITALIAN HOSPITAL COVID-19 WARD appeared first on The anesthesia consultant.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
SANTA CLARA COUNTY, CALIFORNIA Questions I’m frequently asked are, “What is the coronavirus census in your hospital?” or “How full is your hospital with COVID patients?” The first green circle highlights that Stanford Hospital had a total of 15 COVID patients, and there were only 8 COVID patients in the ICU.
Paper-based anesthesia record-keeping is fraught with problems. By automatically capturing data from various devices, and through seamless interoperability with EMR systems, anesthesia information management systems (AIMS) provide a reliable, defensible, accurate and legible record that benefits hospitals, doctors and patients alike.
By addressing these factors, prehabilitation aims to boost the patient’s resilience and functional capacity, enabling them to recover more swiftly and effectively post-surgery. The post Surgical Prehabilitation appeared first on Ambulatory Anesthesia Services | OBS Anesthesia Management Groups.
Though all APRNs undergo extensive training to achieve their advanced degree, each type obtains a different skillset, with CRNAs focused on anesthesia care. In contrast to other APRNs, CRNAs are specially trained to provide anesthesia to patients in settings such as hospitals, clinics, private practices, and doctors’ offices.
Ahead of a visit to the hospital for a surgical procedure, patients often have plenty of questions about what to expect — and can be plenty nervous. These virtual teammates can have natural, human-like conversations with patients, answer a wide range of questions and provide supporting guidance prior to preadmission appointments at hospitals.
Annual meeting Vice-Chair Dr. Engy Said put together a fantastic point-of-care ultrasound and regional anesthesia workshop on Thursday. Mason as well as some other inspirational anesthesiologists, see these video interviews posted by Dr. Allison Fernandez for the Women of Impact in Anesthesiology project. Michael Champeau!
Lidocaine is an amide local anesthetic commonly used for local or topical anesthesia. Intravenous lidocaine also appeared to have advantageous effects [RJ1] on gastro-intestinal motility, length of hospital stays, postoperative nausea, and opioid consumption. Because of these benefits, Chu et al. JCM 2022 , 11 (12), 3543.
Reducing drug waste created by anesthesiologists can result in significant cost savings for ASC’s and hospitals. Drug waste is a significant contributor to the cost of routine anesthesia care,” said lead author of study Raj Patel, BS, a medical student at University of Illinois Chicago.
Sixty-six percent of surgeries in the United States take place as an outpatient , and many of these surgeries are performed at freestanding facilities distant from hospitals. If the patient is unstable, a physician, usually an anesthesiologist, will need to accompany the patient and the EMTs to the hospital emergency room.
The main questions as to whether a hospital or an ambulatory surgery center can resume elective surgery as of May 2020 are: What is the incidence of COVID-19 in your geographic area? When I’m at Stanford Hospital or the surgery centers in our area I’m confident the environment is safe.
My name is Dr. Richard Novak, the author of About The Anesthesia Consultant. The Anesthesia Consultant exists to increase your knowledge about anesthesia and the practice of medicine before, during, and after surgery. This anesthesia blog contains more than 180 distinct pages and posts, all written by me.
You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5%
Today’s post demonstrates making a reusable N95 mask from common inexpensive operating room supplies. The video is posted here. The required parts are an operating room anesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps.
Richard Novak, an Adjunct Clinical Professor of Anesthesiology at Stanford University Medical Center, is available for anesthesia expert witness consultation. Chemistry, Magna Cum Laude, Carleton College 1976-80 M.D., Chemistry, Magna Cum Laude, Carleton College 1976-80 M.D.,
Post-Anesthesia Care Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operating room and continues until they are stable enough to recover at home or in a hospital room.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The hospital was Watertown Regional Medical Center, located in Watertown, Wisconsin , population 23,861, midway between Milwaukee and Madison. In a word, no. See this link.
Primary Consultant Anesthesiologist The “Preoperative Evaluation” chapter in our Bible, Miller’s Anesthesia , is 80 pages long—one of the longest chapters in the book. It’s almost June, and hundreds of anesthesia residents are about to graduate from residency programs. Read on and I’ll explain why. His clinic resulted in 87.9%
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
Round up your smartest engineer buddies and invent the electronic medical recordkeeping system every hospital needs. Doctors and hospitals who failed to adopt a government-approved EMR system by the end of 2014 faced cutbacks in their Medicare reimbursements. hospitals have an EMR system. How can a hospital recoup this cost?
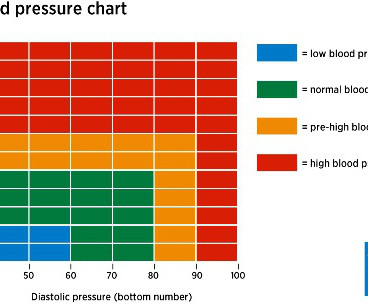
In the operating room, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Anesthesia personnel will be in great demand.
If you wonder how much the anesthesia scene has changed significantly over the past four decades, check out this narrative: In 1986 I was in my second and final year of anesthesia residency training at Stanford, and I was looking for a job. I heard about an opening with a busy private practice anesthesia group in Southern California.
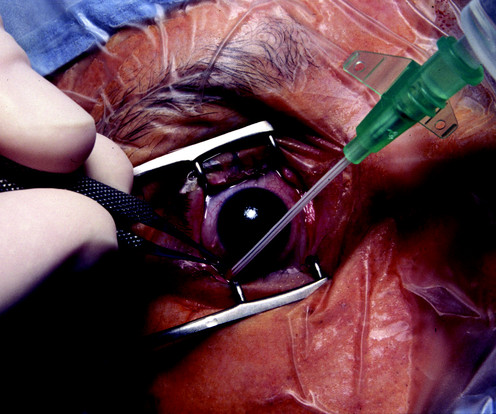
The boy suffers a penetrating open eye injury, and is taken to the nearest hospital. You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. How does a group determine whether a potential anesthesia hire is an affable, friendly, easy-to-get-along-with individual?
In a past column I identified the EHR as the most overrated advance affecting anesthesia practice in the past 25 years. I agree with him that the current cumbersome EHRs come between doctors and patients during hospital care. My criticisms include: Different EHRs at different hospitals are unable to communicate with each other.
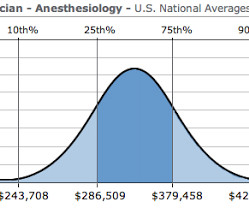
Let me begin by offering two anecdotes: I was an invited visiting anesthesia professor at a major university this year, and following one of my lectures an anesthesiology resident approached me for a discussion. The demand for anesthesia services will grow. How much money does an anesthesiologist earn? It depends.
For non-anesthesiologists, who will not undergo three years of anesthesia residency training to become DL experts, learning video laryngoscopy instead of direct laryngoscopy makes sense. The KISS (Keep It Simple Stupid) Principle is a valuable concept in aviation as well as anesthesia. McGrath blades.
Meanwhile, back at the metaphor, anesthesiologists practiced their essential healing profession, and hoped HMOs and hospital administrators would not decrease their anesthesia quantum wage any further. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From General Anesthesia?
The Merriam-Webster online dictionary defines private practice as: “a professional business (such as that of a lawyer or doctor) that is not controlled or paid for by the government or a larger company (such as a hospital).” A private practice anesthesia group needn’t be a physician-only group. Let’s look at the issues. It depends.
The website was born in 2010 when I posted multiple columns I originally wrote for the Stanford Anesthesia Department publication The Gas Pipeline. Over the following months I added a series of columns aimed at laypeople, answering frequently asked questions about anesthesia. Will I Have a Breathing Tube During Anesthesia?
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
According to an American Hospital Association (AHA) survey of community hospitals, nearly 50% of responding hospitals reported at least 21 drug shortages within the first 6 months of 2011, and more than 99% of hospitals reported at least 1 drug shortage within the same time period. min for ciprofol and 0.80 Anesth Prog.
Anesthesia departments are crucial to the success of operating rooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Here are five warning signs that your anesthesia team might be underperforming: 1.
Peripheral nerve blocks are a type of regional anesthesia that involve injecting local anesthetics and other painkillers near specific nerves or groups of nerves. However, the long-term cost-effectiveness may favor peripheral nerve blocks in some surgical settings due to their potential to reduce hospital stay and opioid use.
Or is it an expensive gadget for hospitals and surgeons to market and attract potential patients? Anesthesia for laparoscopy was similar to the anesthetic for open abdominal surgery. Sixty hospitals in the United States used the system in 2002, but this number grew to 431 hospitals by 2014.
I completed two residencies in the 1980s at Stanford University Hospital, the first in internal medicine and the second in anesthesiology. I worked 30-hour shifts in the hospital every third night on most rotations, without a day off afterwards. The anesthesia residency was 80 hours per week with in-hospital night call.
An anesthesia emergency occurs without warning. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group. Your patient’s vital signs are dropping.
Sugammadex reversal can make the duration of a rocuronium motor block almost as short acting as a succinylcholine motor block, and sugammadex can also eliminate complications in the PostAnesthesia Care Unit due to residual postoperative muscle paralysis. ANESTHESIA ELECTRONIC MEDICAL RECORDS (EMRs)– The idea is sound.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content