This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
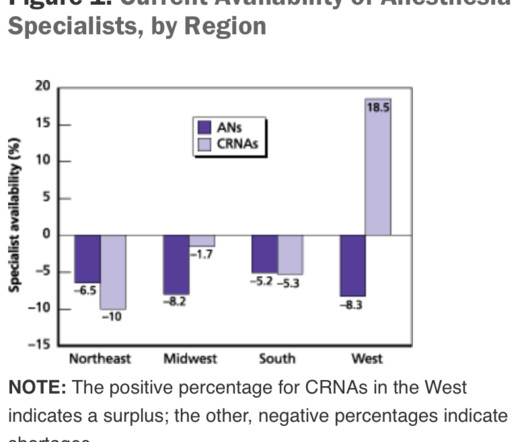
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. Imagine this: It’s the year 2034.
Anesthesia vital signs monitor display A second and more compelling use for smart glasses would be the display of a patient’s vital sign monitoring in real time on the smart glass screen, so that an anesthesiologist is in constant contact with the images of the vital sign electronic monitors. Will I Have a Breathing Tube During Anesthesia?
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10. The patient will probably already have an IV in their arm, placed by a registered nurse. (To
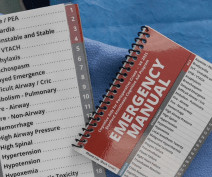
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. A printable version of the Stanford Emergency Manual is available online for free.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). It’s also not uncommon for the patient to be breathing room air during transport.
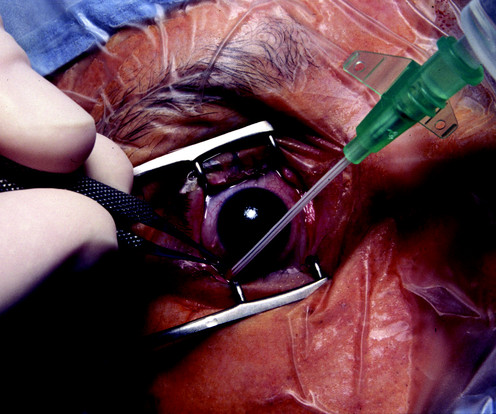
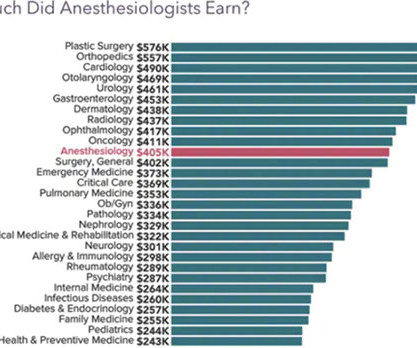
Anesthesiologists still work in hospital operatingrooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. The job of a certified nurse anesthetist was listed as #11 on the Best Paying Jobs list. What Are the Common Anesthesia Medications?
He is verbal with his mother, but refuses to interact with the anesthesia or nursing personnel. The two hospital guards and the mother donned white operatingroom coveralls. Parents often ask about the risk of generalanesthesia to the brain of their child. Will I Have a Breathing Tube During Anesthesia?
When you enter the healthcare facility, a nurse will question you regarding virus symptoms, and will screen you by taking your temperature. The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom.
A doctor or a nurse? On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists typically spend 90+% of their working hours in the operatingroom.
3 Ways Surgical Providers Improve Patient Outcomes Surgical providers—surgical assistants, nurses, and surgical technologists—provide aid during surgery to doctors. Minimize patient time under anesthesiaGeneralanesthesia induces a sleep-like state using a combination of intravenous medications and inhaled gasses.
That’s why we have circulating nurses in the OR.” said Willing Accomplice, the room’s circulating nurse. Shortly after, the spinal anesthetic wore off and the patient was quickly placed under generalanesthesia. Dr. Annuloplasty remains in a ketamine-induced haze in the corner of the operatingroom.
You have to get along well with surgeons, the nursing staff, the scrub techs, administrators, and the patients. Their patients are obtunded on arrival to the Post Anesthesia Care Unit (PACU) after surgery, and they rely on the PACU nursing staff to complete the job of anesthesia wake up. Be friendly and personable.
No one wants a partner who repeatedly creates conflict in the workplace, who initiates conflict with a surgeon in the operatingroom, a nurse in the post anesthesia care unit, or an administrator. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom?
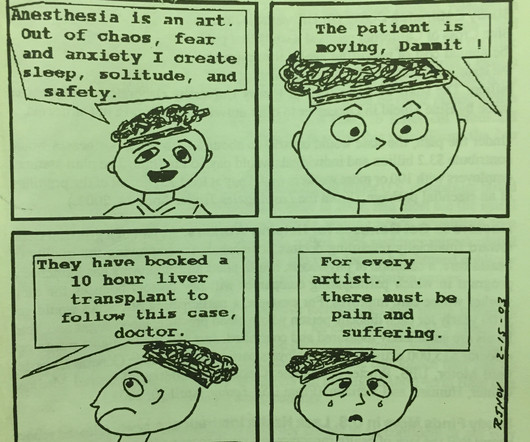
Baker is doing in panel 4, but the anesthesiologist’s rapid heart rate and the adrenaline rush in high pressure operatingroom situations accompany the growth of every anesthesiologist from inexperience trainee to seasoned professional. Why Did Take Me So Long To Wake From GeneralAnesthesia?
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. Nurses consistently have their backs to patients as they type, type, type data into computer terminals.
The da Vinci surgeon sits at a console in the corner of the operatingroom, with his back to the patient and his face in a 3-D viewer, which gives a high-definition, magnified view of the surgical site. Assistant surgeon(s) and techs stand at the patient’s side, watch the surgery on video screens, and assist during the operation.
A private practice anesthesia group needn’t be a physician-only group. In many private practice anesthesia groups, physician anesthesiologists supervise multiple nurse anesthetists in multiple operatingrooms. These groups are still single specialty anesthesia groups.
For a long operatingroomanesthesia case (e.g. Propofol administration requires an experienced clinician, e.g. either an anesthesiologist, a certified registered nurse anesthetist (CRNA), or an emergency medicine physician. Give your patient a dose of Versed before they enter the operatingroom.
My career has bridged clinics, operatingrooms, intensive care units, emergency rooms, and helicopter trauma medicine. In the 21 st century operatingroom practice of anesthesiology, we typically have ten minutes to talk to a patient prior to rendering them unconscious. What Are the Common Anesthesia Medications?
You’ll become rich, and America’s doctors, nurses, and patients will bow to your achievement. Alas, doctors and nurses serve as data-entry technicians for the EPIC system of billing. EPIC is a poor system for doctors and nurses working in a hospital. Why Did Take Me So Long To Wake From GeneralAnesthesia?
More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. What Are the Common Anesthesia Medications?
How can it be that generalanesthesia has ceased to evolve? Anesthesia in 2018 is markedly different from anesthesia in the 1990s. Most of the drugs in use haven’t changed, but current-day anesthesia providers practice in a cockpit surrounded by computers. Why Did Take Me So Long To Wake From GeneralAnesthesia?
When a patient decompensates emergently at a freestanding ambulatory surgery center or in an operatingroom at a doctor’s office, the facility will call for an ambulance staffed with EMT personnel. The surgery was done in a small community hospital where there was no ICU, blood bank, or emergency room.
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% Why Did Take Me So Long To Wake From GeneralAnesthesia?
Unless the hospital is very large, it’s uncommon to have anesthesiologists of multiple specialties on call each day, e.g. one for pediatrics, one for cardiac cases, one for trauma, one for obstetrics, and one for the generaloperatingrooms. Why Did Take Me So Long To Wake From GeneralAnesthesia?
This likely would lead to an increased role for certified nurse anesthetists (CRNAs), and an eventual increase in the number of schools training CRNAs, but in the short term there would be no way to staff adequate numbers of anesthesia professionals. Risk during an anesthesia career is omnipresent.
The teams included plastic surgeons, anesthesiologists, pediatricians, and nurses experienced in the care of cleft palate reconstructions. We started intravenous lines after the induction of anesthesia, but we had very few medications to inject into those IVs. Why Did Take Me So Long To Wake From GeneralAnesthesia?
An operatingroomanesthesia practice is somewhat akin to being a taxi cab driver. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia? Why Did Take Me So Long To Wake From GeneralAnesthesia?
Who is the Captain of the Ship in the operatingroom, the surgeon or the anesthesiologist? The Captain of the Ship doctrine was a 20 th century legal doctrine which held that, in an operatingroom, the surgeon was “liable for all actions conducted in the course of the operation.”
Just before the start of anesthesia, a patient may hear the operatingroomnurse saying, “Think of a nice dream as you go off to sleep.” While these statements are intended to soothe patients during a stressful time, they gloss over this critical fact: Anesthesia is not like normal sleep at all.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The patient enters the operatingroom at 0730 hours. The patient consents.
Anesthesiologists are likely to have: A preference for being in an operatingroom rather than in a clinic. Most of the time an anesthesiologist works in the operatingroom. A busy surgeon may work in the operatingroom two or three days per week. Operatingroom medicine requires action.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). Why Did Take Me So Long To Wake From GeneralAnesthesia?
Will it be a nurse or will it be a physician? Very few patients die in the operatingroom, but significant numbers die in the weeks that follow. At times, physician anesthesiologists employ certified registered nurse anesthetists (CRNAs) to assist them in what is called the anesthesia care team (ACT) model.
But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. No, it’s not the nurse anesthetists, nor the stress of covering surgeries in the middle of the night, nor the stress of saving patients who are trying to die in front of our eyes during acute care emergencies. What is this threat?
Anesthesiologists work in operatingrooms and intensive care units—acute care settings which demand vigilance, steady hands, and quick thinking. These arenas will be: 1) diagnosis of images, 2) clinics, and 3) operatingrooms/intensive care units. Why Did Take Me So Long To Wake From GeneralAnesthesia?
GENERALANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Potent inhalation anesthesia (sevoflurane). What do you do?
Louis Imagine this: You’re an anesthesiologist in the operatingroom at a busy hospital. Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger.
On the 1 – 3 days a week most surgeons spend operating, they are joined in the operatingroom by anesthesiologists who attend to surgical patients’ lives every day. TOP 10 MOST STRESSFUL SITUATIONS IN AN ANESTHESIOLOGIST’S JOB Emergency generalanesthesia in a morbidly obese patient. Picture a 3 a.m.
In an anesthesia care team, a physician anesthesiologist supervises up to four operatingrooms and each operatingroom is staffed with a certified registered nurse anesthetist (CRNA). In many hospital operatingrooms, a solitary physician anesthesiologist attends to his or her patient alone.
Are we physicians or are we glorified advanced practice nurses?” In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operatingroom. Read my column on bullying in the operatingroom. He or she knows how to do the operation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content