This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
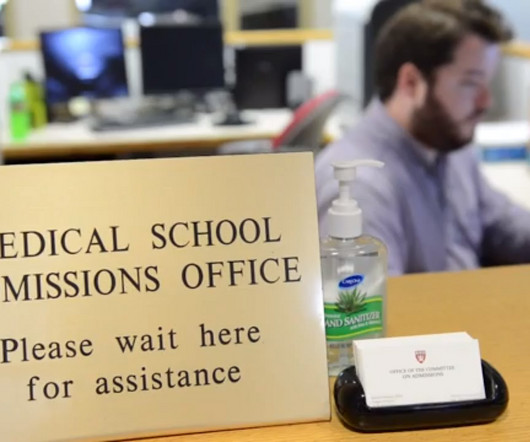
What’s the difference between a physician anesthesiologist and a nurseanesthetist? After the first 3 – 4 years in the workforce, either one can master the manual skills of anesthesia. So what really is the difference between a physician anesthesiologist and a nurseanesthetist? The answer: internal medicine.
Does exposure to generalanesthesia cause dementia? Association of Mild Cognitive Impairment With Exposure to GeneralAnesthesia for Surgical and Nonsurgical Procedures: A Population-Based Study. All of their anesthesia records for surgeries after the age of 40 were reviewed. In a word, “No.” Anesthesiology.
An anesthesia colleague wrote to me several months ago, asking for my recommendations for achieving smooth emergence. I’ve performed countless general anesthetics for surgeries requiring smooth emergence, specifically carotid endarterectomies, rhinoplasties, facelifts, craniotomies, thyroidectomies, and other head and neck procedures.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
Most anesthesiology residents go on to do a one- to two-year fellowship program to learn a subspecialty, such as critical care or obstetric anesthesia. The job of a certified nurseanesthetist was listed as #11 on the Best Paying Jobs list. Why Did Take Me So Long To Wake From GeneralAnesthesia?
My name is Dr. Richard Novak, the author of About The Anesthesia Consultant. The Anesthesia Consultant exists to increase your knowledge about anesthesia and the practice of medicine before, during, and after surgery. This anesthesia blog contains more than 180 distinct pages and posts, all written by me.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered NurseAnesthetists). Why did this change happen?
Meanwhile, back at the metaphor, anesthesiologists practiced their essential healing profession, and hoped HMOs and hospital administrators would not decrease their anesthesia quantum wage any further. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. For insured patients, the anesthesia group collects whatever the insurance company pays, along with the deductible or co-pay the patient owes through their insurance plan.
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurseanesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. In a perfect anesthesia world, patients will not move.
More care team anesthesia and more Certified NurseAnesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. Anesthesia has never been safer.
Regional anesthesia is a growing frontier in modern clinical anesthesia, in part because of the availability of ultrasonic imaging to help us direct needle placement. The subspecialty of regional anesthesia has blossomed. following generalanesthesia in contrast to a peripheral nerve injury rate of 1.7%
We learn those skills, and then we pass the American Board of Anesthesia written and oral exams on these skills. Then for the rest of our careers we lose many anesthesia skills. Every year in June across the United States another class of anesthesia residents finishes training. In the 1990’s the rock group R.E.M. Very common.
Point/Counterpoint: How new is modern anesthesia? Are modern anesthesia techniques radically different from the methods of twenty years ago? Twenty-first century general anesthetics are nearly identical to the anesthetic techniques of the late 1990s. How can it be that generalanesthesia has ceased to evolve?
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. Why Did Take Me So Long To Wake From GeneralAnesthesia? What Are the Common Anesthesia Medications?
I commonly hear two questions from my patients: “How does anesthesia work?” Generalanesthesia is the sum of hypnosis (sleep), amnesia, analgesia (pain relief), and the lack of any motion response to pain. Why Did Take Me So Long To Wake From GeneralAnesthesia? Will I Have a Breathing Tube During Anesthesia?
Sugammadex reversal can make the duration of a rocuronium motor block almost as short acting as a succinylcholine motor block, and sugammadex can also eliminate complications in the PostAnesthesia Care Unit due to residual postoperative muscle paralysis. ANESTHESIA ELECTRONIC MEDICAL RECORDS (EMRs)– The idea is sound.
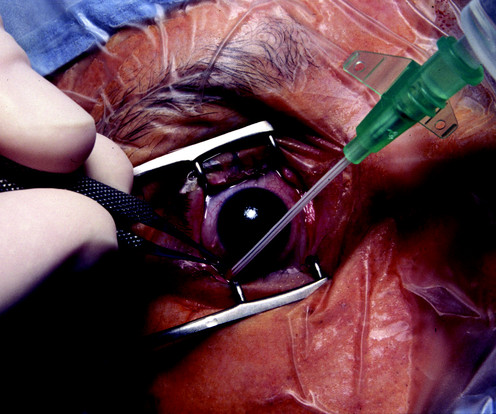
You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists. Why Did Take Me So Long To Wake From GeneralAnesthesia?
My aim is to inform my readers, both anesthesia professionals and laypersons, that if Medicare for All becomes reality, there will be a dire consequence regarding anesthesia staffing and services to patients. What happens if every anesthesia patient pays only Medicare rates in a Medicare for All future? 75 X $76) + (.25
Anesthesia vital signs monitor display A second and more compelling use for smart glasses would be the display of a patient’s vital sign monitoring in real time on the smart glass screen, so that an anesthesiologist is in constant contact with the images of the vital sign electronic monitors. Let me give you a historical perspective.
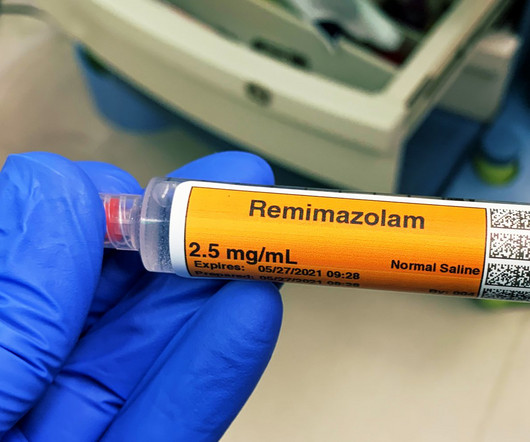
The only way to end the sedative effects of propofol is for an anesthesia professional to support the airway, breathing, and circulation of the patient until the drug effects of propofol wear off in time. I’ve never administered a dose of flumazenil in my entire career, nor have most of my anesthesia colleagues.
The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia? Why Did Take Me So Long To Wake From GeneralAnesthesia? Will I Have a Breathing Tube During Anesthesia? What Are the Common Anesthesia Medications?
Let me begin by offering two anecdotes: I was an invited visiting anesthesia professor at a major university this year, and following one of my lectures an anesthesiology resident approached me for a discussion. The demand for anesthesia services will grow. How much money does an anesthesiologist earn? It depends.
Nowadays when patients arrive at the hospital for surgery, it’s not uncommon for them to be armed with abundant information on their disease, their pending operation, and even their anesthesia options. Anyone can put medical information on a Web server, and the information posted may be incorrect or outdated.
I stay with the child until the anesthetic depth has dissipated, the breathing tube is removed, and the child is awake and safe with the recovery room nurse in the PostAnesthesia Care Unit. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists. These results complement previous studies that have shown improved 30-day mortality and morbidity rates after complications when anesthesiologists directed anesthesia care.” Figure 3: 7 a.m.
A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. Planning anesthesia care, based on your training, experience, and knowledge, is critical.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Anesthesia Workstation You log into the EMR system, and then you log into your first patient’s chart. The lower drawers to the computerized pharmacy cart unlock, and you’re able to access the propofol you’ll use to induce anesthesia.
Prior to surgery your patient tells you, “I always get a hangover after generalanesthesia. Hangover after generalanesthesia (HAGA) describes a patient who has a safe general anesthetic, but who then feels hungover, sedated, and wasted for a time period exceeding two hours afterwards. The patient is always right.
Anesthesiology is a wonderful profession, as I have described in many previous posts on theanesthesiaconsultant.com. But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. Anesthesia providers are at best consultants, and at worst, “worker bees” called upon to provide a service.
This technique induced vasoconstriction and resulted in decreased blood loss, and made transfusion and post-operative anemia rare. The procedures are done under general endotracheal anesthesia, and can last from 3 to 8 hours. A protocol for large-volume liposuction at our facility is as follows: Generalanesthesia is induced.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). If the patient has an ET tube, it is usually removed.
. * * * * LEARN MORE ABOUT RICK NOVAK’S FICTION WRITING AT RICK NOVAK.COM BY CLICKING ON THE PICTURE BELOW: The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia? Why Did Take Me So Long To Wake From GeneralAnesthesia?
Anesthesia is a hands-on specialty. Anesthesia is said to be “99% boredom and 15 panic,” because 99% of the time patients are stable, yet 1% of the time, especially at the beginning and the end of anesthetics, urgent or emergency circumstances could threaten the life of the patient. Love it or hate it, the EMR is here to stay.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. What went wrong?
I ask this question when I’m teaching anesthesia residents and medical students. Control of the airway is the most important clinical priority in anesthesia care. The INTUBATION AFTER INDUCTION OF GENERALANESTHESIA section of the Difficult Airway Algorithm is bifurcated into two pathways. Their most frequent answer is.
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. INTRAOPERATIVE DECISION A 60-year-old man with a history of hypertension is having a knee arthroscopy surgery under generalanesthesia. Is CHATGPT as good as an MD? No, not really.
GENERALANESTHESIA FOR DENTAL OFFICES CASE PRESENTATION: A 5-year-old developmentally delayed autistic boy has multiple dental cavities. The dentist consults you, a physician anesthesiologist, to do sedation or anesthesia for dental restoration. Options for anesthesia induction include: Intramuscular sedation.
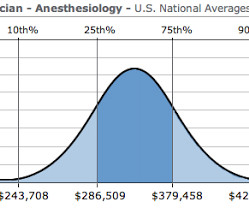
How do you feel when you meet your anesthesia provider prior to a surgical procedure? In an abstract presented at the 2015 American Society of Anesthesiologists annual meeting, data from the 2014 National Anesthesia Clinical Outcomes Registry was compiled for every anesthesiologist of known age who performed at least 100 cases.
See Robot Anesthesia and Robot Anesthesia II ) AI already influences our daily life. In my previous essays Robot Anesthesia and Robot Anesthesia II , I described models of robots designed to perform intravenous sedation or intubation of the trachea, products which are futuristic but currently have no market share.
Your patient is in mid-surgery, and you receive a call from the Anesthesia Control Tower that the patient’s blood pressure is too low, your blood transfusion replacement is inadequate, and that the patient is in danger. Louis, Missouri are studying a novel system they call the Anesthesia Control Tower (ACT). What do you do?
What should you do if your 2-year-old son or daughter requires surgery and anesthesia? Anesthesia for infants and children is most frequently initiated with an inhalation induction of sevoflurane vapor, because most infants and children do not have an IV line prior to induction. What are the anesthetic risks for children?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content