This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Perioperative hypothermia, defined as a core body temperature below 36°C, is a frequent and preventable complication associated with anesthesia and surgical procedures. The post-operative phase is crucial for reinforcing normothermia and supporting patient recovery, yet it is often overlooked in thermal management. BMC Anesthesiol.
Does exposure to generalanesthesia cause dementia? Association of Mild Cognitive Impairment With Exposure to GeneralAnesthesia for Surgical and Nonsurgical Procedures: A Population-Based Study. All of their anesthesia records for surgeries after the age of 40 were reviewed. In a word, “No.” Anesthesiology.
An anesthesia colleague wrote to me several months ago, asking for my recommendations for achieving smooth emergence. I’ve performed countless general anesthetics for surgeries requiring smooth emergence, specifically carotid endarterectomies, rhinoplasties, facelifts, craniotomies, thyroidectomies, and other head and neck procedures.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
My name is Dr. Richard Novak, the author of About The Anesthesia Consultant. The Anesthesia Consultant exists to increase your knowledge about anesthesia and the practice of medicine before, during, and after surgery. This anesthesia blog contains more than 180 distinct pages and posts, all written by me.
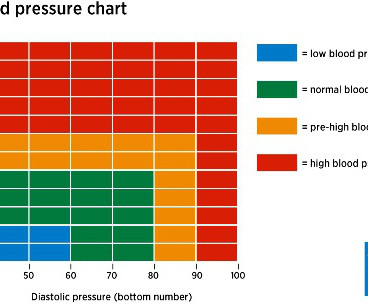
In the operating room, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
Sixty-six percent of surgeries in the United States take place as an outpatient , and many of these surgeries are performed at freestanding facilities distant from hospitals. If the patient is unstable, a physician, usually an anesthesiologist, will need to accompany the patient and the EMTs to the hospital emergency room.
The website was born in 2010 when I posted multiple columns I originally wrote for the Stanford Anesthesia Department publication The Gas Pipeline. Over the following months I added a series of columns aimed at laypeople, answering frequently asked questions about anesthesia. Will I Have a Breathing Tube During Anesthesia?
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
Meanwhile, back at the metaphor, anesthesiologists practiced their essential healing profession, and hoped HMOs and hospital administrators would not decrease their anesthesia quantum wage any further. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
The main questions as to whether a hospital or an ambulatory surgery center can resume elective surgery as of May 2020 are: What is the incidence of COVID-19 in your geographic area? When I’m at Stanford Hospital or the surgery centers in our area I’m confident the environment is safe.
Anesthesiologists still work in hospital operating rooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. Careers in anesthesia are intellectually stimulating, emotionally gratifying, and have high median salaries and ultra-low unemployment.
Richard Novak, an Adjunct Clinical Professor of Anesthesiology at Stanford University Medical Center, is available for anesthesia expert witness consultation. Chemistry, Magna Cum Laude, Carleton College 1976-80 M.D., Chemistry, Magna Cum Laude, Carleton College 1976-80 M.D.,
If you wonder how much the anesthesia scene has changed significantly over the past four decades, check out this narrative: In 1986 I was in my second and final year of anesthesia residency training at Stanford, and I was looking for a job. I heard about an opening with a busy private practice anesthesia group in Southern California.
According to an American Hospital Association (AHA) survey of community hospitals, nearly 50% of responding hospitals reported at least 21 drug shortages within the first 6 months of 2011, and more than 99% of hospitals reported at least 1 drug shortage within the same time period. min for ciprofol and 0.80 Anesth Prog.
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Anesthesia personnel will be in great demand.
Ability can also be evidenced the quality of the anesthesia residency/fellowship training program you’ve completed, as well as the medical school you’ve graduated from. How does a group determine whether a potential anesthesia hire is an affable, friendly, easy-to-get-along-with individual?
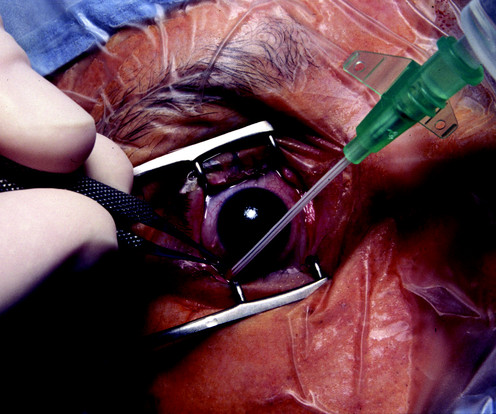
The boy suffers a penetrating open eye injury, and is taken to the nearest hospital. You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists.
Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. In many health care systems there are no anesthesia clinics, and primary care doctors (internal medicine specialists, family practitioners, or pediatricians) do the preoperative assessments.
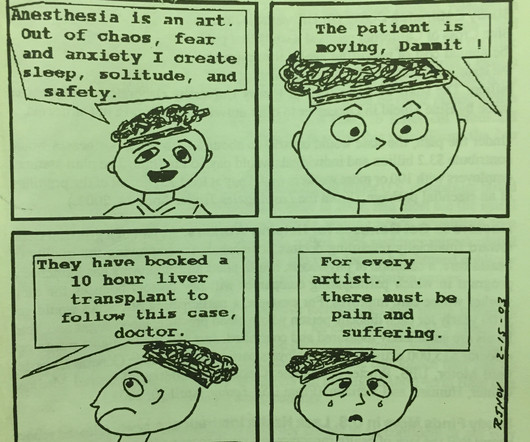
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
In a past column I identified the EHR as the most overrated advance affecting anesthesia practice in the past 25 years. I agree with him that the current cumbersome EHRs come between doctors and patients during hospital care. My criticisms include: Different EHRs at different hospitals are unable to communicate with each other.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The hospital was Watertown Regional Medical Center, located in Watertown, Wisconsin , population 23,861, midway between Milwaukee and Madison. In a word, no. See this link.
But one large subset of anesthesia work closely mimics the lifestyle of dermatology practice. Ambulatory anesthesiology is defined as the administration of anesthetics for outpatient surgical procedures, which are minor procedures which don’t require hospitalization. Anesthesia will never be as safe or predictable as dermatology.
For non-anesthesiologists, who will not undergo three years of anesthesia residency training to become DL experts, learning video laryngoscopy instead of direct laryngoscopy makes sense. The KISS (Keep It Simple Stupid) Principle is a valuable concept in aviation as well as anesthesia. McGrath blades.
I completed two residencies in the 1980s at Stanford University Hospital, the first in internal medicine and the second in anesthesiology. I worked 30-hour shifts in the hospital every third night on most rotations, without a day off afterwards. The anesthesia residency was 80 hours per week with in-hospital night call.
Point/Counterpoint: How new is modern anesthesia? Are modern anesthesia techniques radically different from the methods of twenty years ago? Twenty-first century general anesthetics are nearly identical to the anesthetic techniques of the late 1990s. How can it be that generalanesthesia has ceased to evolve?
Regional anesthesia is a growing frontier in modern clinical anesthesia, in part because of the availability of ultrasonic imaging to help us direct needle placement. The subspecialty of regional anesthesia has blossomed. following generalanesthesia in contrast to a peripheral nerve injury rate of 1.7%
The video provides answers to individuals who have obstructive sleep apnea and are contemplating surgery and anesthesia. Patients with OSA frequently present for surgery, and all anesthesia professionals must be aware of the risks involved with anesthetizing OSA patient. Risks of anesthesia and the OSA patient?
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? Should you buy these books, or should you advocate that your hospital purchase them for the medical library? All anesthesia providers should have access to the current two-volume 3112-page edition.
You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% The patient objects.
The Merriam-Webster online dictionary defines private practice as: “a professional business (such as that of a lawyer or doctor) that is not controlled or paid for by the government or a larger company (such as a hospital).” A private practice anesthesia group needn’t be a physician-only group. Let’s look at the issues. It depends.
What’s the relationship between alcohol and anesthesia? Miller’s Anesthesia , 9 th edition, Chapter 31, Preoperative Evaluation) All adults and adolescents should be questioned regarding their history of alcohol use prior to anesthesia. Why Did Take Me So Long To Wake From GeneralAnesthesia? Is this OK?
An anesthesia emergency occurs without warning. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group. Your patient’s vital signs are dropping.
The Stanford Emergency Manual has been used in all Stanford Hospital anesthetizing locations since 2012, and Stanford has printed and shipped thousands of Manuals to institutions around the United States and the world. Both were published in the journal Anesthesia and Analgesia. Why Did Take Me So Long To Wake From GeneralAnesthesia?
At that age you’ll have a negative net worth, and you’ll be financially years behind your friends who went to work immediately out of college You’ll work long hours, including sleeping overnight in hospitals during your training. Answering phone calls or being summoned into the hospital at 3 a.m. 80-hour work weeks are common.
Primary Consultant Anesthesiologist The “Preoperative Evaluation” chapter in our Bible, Miller’s Anesthesia , is 80 pages long—one of the longest chapters in the book. It’s almost June, and hundreds of anesthesia residents are about to graduate from residency programs. Read on and I’ll explain why. His clinic resulted in 87.9%
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. In a perfect anesthesia world, patients will not move.
If you’re wondering how your hospital or surgery center could benefit from the integration of these professionals, here are three ways that they improve patient outcomes. Minimize patient time under anesthesiaGeneralanesthesia induces a sleep-like state using a combination of intravenous medications and inhaled gasses.
I commonly hear two questions from my patients: “How does anesthesia work?” Generalanesthesia is the sum of hypnosis (sleep), amnesia, analgesia (pain relief), and the lack of any motion response to pain. Why Did Take Me So Long To Wake From GeneralAnesthesia? Will I Have a Breathing Tube During Anesthesia?
Round up your smartest engineer buddies and invent the electronic medical recordkeeping system every hospital needs. Doctors and hospitals who failed to adopt a government-approved EMR system by the end of 2014 faced cutbacks in their Medicare reimbursements. hospitals have an EMR system. How can a hospital recoup this cost?
How soon will we see robotic anesthesia in our hospitals and surgery centers? Most of these discoveries originated in Silicon Valley, just miles outside Stanford University Hospital where I’ve been working for the past 42 years. Our medical world inside the hospital has changed more slowly. Relatively little.
Dr. Gaba developed the anesthesia crisis simulator , and his group developed the Stanford Anesthesia Emergency Manual. Both are landmark contributions toward reducing medical errors by anesthesia providers and improving patient outcomes. Dr. Eisenach is a Professor of Anesthesia at Wake Forest University.
Or is it an expensive gadget for hospitals and surgeons to market and attract potential patients? Anesthesia for laparoscopy was similar to the anesthetic for open abdominal surgery. Sixty hospitals in the United States used the system in 2002, but this number grew to 431 hospitals by 2014.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content