This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Securing admission into a Certified Registered Nurse Anesthetist (CRNA) program is no small feat. With a rapidly growing demand for CRNA professionals and a surge in applicants, the competition has become fiercer than ever before. Ideally, you should begin preparing by researching CRNA programs extensively.
They play a crucial role in healthcare by ensuring patient safety and comfort before, during, and after surgical procedures. To begin, it’s essential to understand the role of a CRNA. CRNAs received specialized training that is critical in surgeries and healthcare.
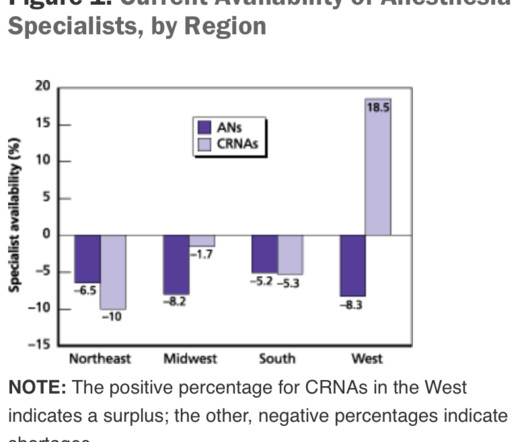
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
Salem Anesthesia is fortunate to have the best Anesthesiologists on our team. Their education, training and expertise is impressive and very appreciated by our surgical centers, CRNA s and patients. Salem Anesthesia truly values the remarkable anesthesiologists in our group! Surgical care is a complex and dynamic effort.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Anesthesia Workstation You log into the EMR system, and then you log into your first patient’s chart. The lower drawers to the computerized pharmacy cart unlock, and you’re able to access the propofol you’ll use to induce anesthesia.
Anesthesia is a hands-on specialty. Anesthesia is said to be “99% boredom and 15 panic,” because 99% of the time patients are stable, yet 1% of the time, especially at the beginning and the end of anesthetics, urgent or emergency circumstances could threaten the life of the patient. Love it or hate it, the EMR is here to stay.
Every anesthesia provider must learn to free-solo anesthesia early in his or her career. The 2018 movie Free Solo showcases Alex Honnold as he became the first person to free solo climb the 3000-feet high El Capitan wall of granite in Yosemite National Park without ropes or safety gear. Working alone may be less safe.
Who is responsible for your safety before, during, and after your surgery? At times, physician anesthesiologists employ certified registered nurse anesthetists (CRNAs) to assist them in what is called the anesthesia care team (ACT) model. Are CRNAs and anesthesiologists equals? This is an important question.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
The study looked at malpractice closed claims and found: 1) Outcomes remained poor in malpractice closed claims related to difficult tracheal intubation; 2) The incidence of brain damage or death at induction of anesthesia was 5.5 This training needs to be a requirement for all anesthesia professionals. Not really.
Last November, two hospitals in Portland, Oregon, reportedly had to cancel several hundred procedures—nearly all nonemergency surgeries—due to a shortage of anesthesia providers. This incident is just one More » The post The anesthesia staffing crisis: How we got here, what hospitals can do appeared first on OR Manager.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content