This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
August 19, 2024 – The Society of Future Nurse Anesthetists (SFNA), a new nonprofit organization dedicated to empowering critical care nurses and aspiring nurse anesthetists, is excited to announce its official launch. GREENVILLE, SC., Objective : Promote holistic health, stress management, and overall wellness.
Transitioning from working as an ICU nurse to becoming a Certified Registered Nurse Anesthetist (CRNA) is a journey marked by immense growth but also profound challenges. ICU nurses are adept at managing complex critical care situations, which provides a solid foundation for a career in anesthesia.
As the Society of Future Nurse Anesthetists (SFNA) emerges from the Facebook Group “Future CRNA Society,” it is crucial to dive into the comprehensive programs and resources that define this transition phase. Our program stands at the core of SFNA’s mission to support the next generation of CRNAs.
Becoming a Certified Registered Nurse Anesthetist (CRNA) is both an exciting and demanding endeavor. Besides the rigorous academic and clinical requirements, prospective CRNAs must also navigate the financial challenges of their education. These costs can vary significantly depending on the program, location, and other factors.
Do you know what it takes to become a Certified Registered Nurse Anesthesiologist (CRNA)? The NurseAnesthesia school admissions process is extraordinarily time-consuming and highly competitive and anyone considering this path should expect it to take a number of years.
What was once known as The CRNA Chase Academy will now be proudly recognized as The Society of Future Nurse Anesthetists (SFNA). This transition marks a new chapter in our commitment to supporting critical care nurses and aspiring nurse anesthetists on their professional journeys. Why the Change?
The journey to becoming a Resident Registered Nurse Anesthetist (RRNA) is both time-consuming and highly competitive. The admissions process for NurseAnesthesia programs is rigorous and can take several years. The future for CRNAs looks promising, with a predicted employment growth of 45% from 2020 to 2030.
Securing admission into a Certified Registered Nurse Anesthetist (CRNA) program is no small feat. With a rapidly growing demand for CRNA professionals and a surge in applicants, the competition has become fiercer than ever before. The competition is fierce, with highly qualified ICU nurses vying for the same spots.
Every year in January, we celebrate CRNA week. Last week, I encounter a patient that I’ve taken care of twice before (how likely is it amongst 30 CRNAs at the hospital that I get to take care of him 3 times in a row?). Another patient required extra TLC, explanations and a calming presence prior to the induction of anesthesia.
This post may contain affiliate links. I’m super excited to talk about one of my favorite topics which is all about how to get accepted to the right CRNA school by standing out from the rest of the crowd. I actually posted it Tuesday and you can go back to Tuesday’s post and get that. I feel your pain.
The Society of Future Nurse Anesthetists (SFNA) is thrilled to unveil some of the new features and benefits designed to empower and support our members on their Certified Registered Nurse Anesthetist (CRNA) journeys. Career resources tailored to nurses and aspiring nurse anesthetists.
Resume And because you do not create a CV often enough and the reason you really don’t create one often enough is because as nurses we actually put everything down on our CV the first time and we leave it and then apply to a job. For this though, we really going for nurseanesthesia, you know physician in the class, right?
All APRNs are registered nurses who have earned a graduate degree that certifies them to practice advanced and specialized care. There are four classes of APRNs: certified nurse midwife (CNM), clinical nurse specialist (CNS), certified nurse practitioner (CNP), and certified registered nurse anesthetist (CRNA).
On behalf of the Pennsylvania Association of Nurse Anesthetists, I want to wish everyone a happy National CRNA Week in Pa.! While CRNA Week is just a snapshot in time, the critical role we play is year-round. Today, there are more than 61,000 practicing CRNAs in the United States.
I have three businesses- my anesthesia services is the main one that I do. My 7:00 to 3:00 Monday through Friday, usually unless I just want to take off and that is Priority First Anesthesia. She is also a CRNA and lives in Kansas now. I mean honestly, that’s kind of how I felt with CRNA school, but I felt called to do it.
A guiding principle of Salem Anesthesia is to treat the surgical centers and patients we serve with the utmost respect, unmatched care and professionalism. Our team of Anesthesiologists and CRNAs have met this goal for over 30 years and welcoming Bradley Quarles to our team will help ensure we continue to do so.
Certified Registered Nurse Anesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. To begin, it’s essential to understand the role of a CRNA. CRNAs received specialized training that is critical in surgeries and healthcare.
CRNA Students Marie Richardson, Nina Marino and ,, Mamawa Hollendyke , MSN, RN received a visit from Pa. s NurseAnesthesia program, sharing their nursing backgrounds and why they were particularly interested in York's program. After discussing the CRNA profession and touring the simulation lab, Sen.
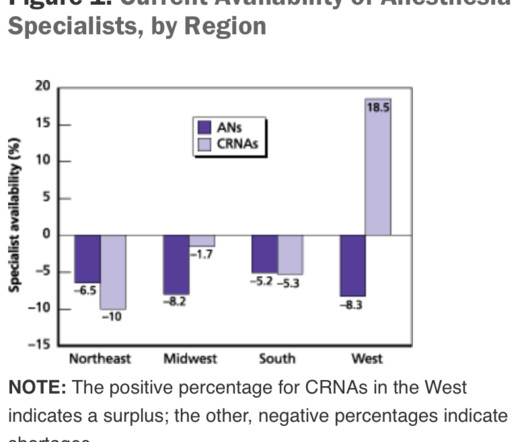
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
What’s the difference between a physician anesthesiologist and a nurse anesthetist? After the first 3 – 4 years in the workforce, either one can master the manual skills of anesthesia. So what really is the difference between a physician anesthesiologist and a nurse anesthetist? The answer: internal medicine.
ICYMI in person, Jeremy Stanley, CFP, AIF and Sharon Pearce, MSN, CRNA sat down with #CRNAinPA Brett Fadgen back on Saturday, May 6th to hear more about his personal story, which includes a timeline of the innovations and opportunities for CRNAs, once believed to be unattainable. 9:05 ) The challenges he faced in anesthesia school. (
Advanced Practice Provider Spotlight: Certified registered nurse anesthetist shares perspective on caring for diverse patients Posted April 11, 2023 by ,Penn State Health News Prolung Ngin , a certified registered nurse anesthetist (CRNA) at Penn State Health Milton S.
A doctor or a nurse? On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “
A nursing degree unlocks a plethora of career opportunities. With an array of jobs you can get with a nursing degree , choosing your path might seem daunting, but it doesn’t have to be. This article aims to simplify your search for nursing degree jobs , shedding light on various nursing roles.
The University of Michigan paper stated, “this study primarily analyzed physician-CRNA teams, the dominant practice model in US anesthesiology.” The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists.
Salem Anesthesia is fortunate to have the best Anesthesiologists on our team. Their education, training and expertise is impressive and very appreciated by our surgical centers, CRNA s and patients. Salem Anesthesia truly values the remarkable anesthesiologists in our group! Surgical care is a complex and dynamic effort.
Are you unhappy with your current anesthesia job? Are you a resident or fellow or a nurse anesthetist looking for your first job? Every week thousands of anesthesiologists and nurse anesthetists are looking for new employment. Internet websites post job advertisements for anesthesia professionals.
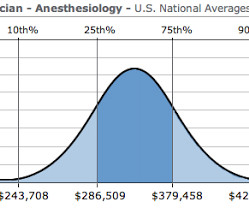
Let me begin by offering two anecdotes: I was an invited visiting anesthesia professor at a major university this year, and following one of my lectures an anesthesiology resident approached me for a discussion. The demand for anesthesia services will grow. How much money does an anesthesiologist earn? It depends.
Most anesthesiology residents go on to do a one- to two-year fellowship program to learn a subspecialty, such as critical care or obstetric anesthesia. The job of a certified nurse anesthetist was listed as #11 on the Best Paying Jobs list. Why Did Take Me So Long To Wake From General Anesthesia?
Sugammadex reversal can make the duration of a rocuronium motor block almost as short acting as a succinylcholine motor block, and sugammadex can also eliminate complications in the PostAnesthesia Care Unit due to residual postoperative muscle paralysis. ANESTHESIA ELECTRONIC MEDICAL RECORDS (EMRs)– The idea is sound.
The only way to end the sedative effects of propofol is for an anesthesia professional to support the airway, breathing, and circulation of the patient until the drug effects of propofol wear off in time. I’ve never administered a dose of flumazenil in my entire career, nor have most of my anesthesia colleagues.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Anesthesia Workstation You log into the EMR system, and then you log into your first patient’s chart. The lower drawers to the computerized pharmacy cart unlock, and you’re able to access the propofol you’ll use to induce anesthesia.
Which is why I created the Facebook group- Future CRNA Society and The CRNA Chase. Just take the difficulty out of it and I want you to think about this whole CRNA journey with intention and make it simple. Watch Full Video on Facebook My Long CRNA Journey Think about 11 Years at $200,000 a year. I was rejected twice.
The operating room team today consists of multiple professionals working in collaboration, including the surgeon, the scrub tech, the circulating nurse, and the anesthesia MD or CRNA. Many surgeons chose to lord over the anesthesia attendings with verbal abuse and a condescending attitude.
Will it be a nurse or will it be a physician? At times, physician anesthesiologists employ certified registered nurse anesthetists (CRNAs) to assist them in what is called the anesthesia care team (ACT) model. Are CRNAs and anesthesiologists equals? This is an important question. No, they are not.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. The surgery concludes at 1630 hours.
Anesthesia is a hands-on specialty. Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operating room. Since the development of the internet, anesthesia practice has changed forever. Love it or hate it, the EMR is here to stay.
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. INTRAOPERATIVE DECISION A 60-year-old man with a history of hypertension is having a knee arthroscopy surgery under general anesthesia. This could indicate a cardiac event or a complication related to the anesthesia.
Every anesthesia provider must learn to free-solo anesthesia early in his or her career. A typical hospital will have dozens of other anesthesia providers working in the same building. Commercial aviation is sometimes compared to anesthesia practice. In anesthesia there is no guaranteed second anesthesiologist.
He writes, “Our specialty, anesthesia, has suffered an identity crisis for decades. Are we physicians or are we glorified advanced practice nurses?” The surgical attendings were the kings, the students were the peasants, the nurses and techs were serfs, and the anesthesiologists were the whipping boys for the surgeons.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of general anesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). If the patient has an ET tube, it is usually removed.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
The study looked at malpractice closed claims and found: 1) Outcomes remained poor in malpractice closed claims related to difficult tracheal intubation; 2) The incidence of brain damage or death at induction of anesthesia was 5.5 This training needs to be a requirement for all anesthesia professionals. What should you do now?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content