This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Who is the Captain of the Ship in the operatingroom, the surgeon or the anesthesiologist? The Captain of the Ship doctrine was a 20 th century legal doctrine which held that, in an operatingroom, the surgeon was “liable for all actions conducted in the course of the operation.”
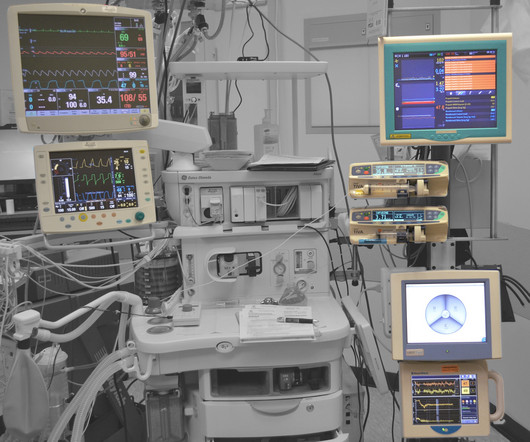
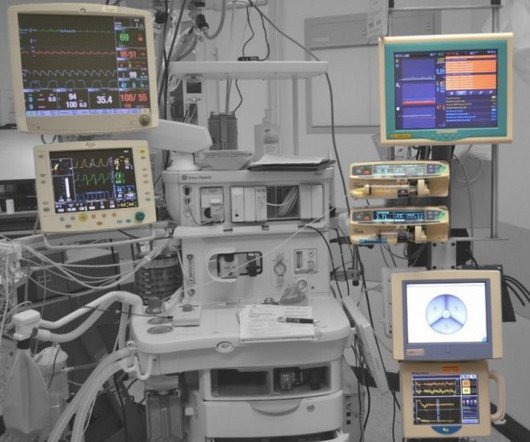
Anesthesiologists watch vital sign monitors continuously in the operatingroom every day, and have more experience following vital sign abnormalities minute-to-minute than other physicians. The blood oxygen level, or oxygen saturation level, is equivalent to what a pulse oximeter measures in the operatingroom.
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
Anesthesiology residents play an important role in the operatingroom (OR), assisting with patient care while also undergoing rigorous training to become skilled anesthesiologists. Their responsibilities encompass a range of tasks, from preoperative evaluations to the administration of anesthesia and postoperative care.
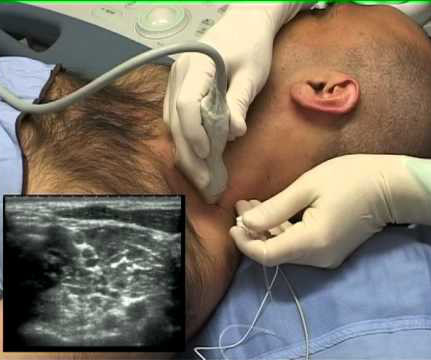
Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. In the control group of this study, each anesthesiologist would use a traditional ultrasound screen to visualize the artery. This was an important study, and important information.
Annual meeting Vice-Chair Dr. Engy Said put together a fantastic point-of-care ultrasound and regional anesthesia workshop on Thursday. Mason as well as some other inspirational anesthesiologists, see these video interviews posted by Dr. Allison Fernandez for the Women of Impact in Anesthesiology project.
In recent years, engineers have developed closed-loop AI machines that can administer appropriate doses of anesthetics without human input , as described in The Washington Post article, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Thus, we might ask, ‘What happens to the operator/clinician involved?’
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). (He Are CRNAs and anesthesiologists equals?
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring.,
What qualities define an outstanding anesthesiologist? A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. This can be a vain conceit.
Is your doctor an experienced anesthesia provider or a newbie? The list below chronicles the crescendo of growth of as I’ve witnessed it from a newly-trained anesthesia doctor to an expert practitioner. In my view, inexperienced anesthesia providers are more likely to: Be nervous/anxious. This observation is no surprise.
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade. Why Did Take Me So Long To Wake From General Anesthesia?
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% The patient does well, and is discharged from the PostAnesthesia Care Unit in excellent condition. He’s right. What happened? What happened?
Will Gawande change the future for anesthesiologists? Let’s look at these three proposed Gawande changes, and how they affect the future for anesthesiologists: Taking out the trash. This proposed elimination of wasteful spending would decrease the demand for anesthesia professionals. Creating a checklist.
There are Two Laws of Anesthesia, according to surgeon lore. Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Most surgeons’ comprehension of what anesthesiologists are doing is limited.
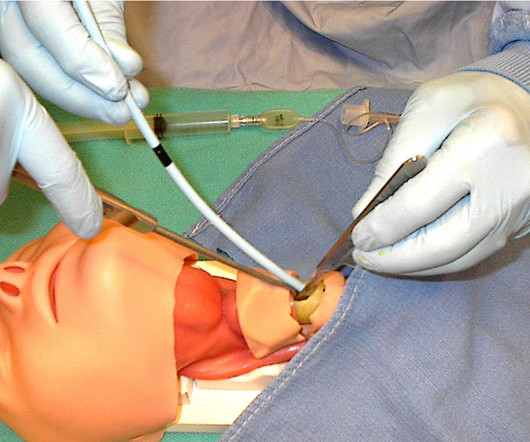
Miller 2 Direct Laryngoscope Video Laryngoscope When it’s time to insert an endotracheal tube, for decades anesthesiologists have utilized a direct laryngoscope. Direct laryngoscopy (DL) is a difficult skill to acquire, but all anesthesiologists become masters of it. Enter the video camera, which changed surgical practice.
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. Both were published in the journal Anesthesia and Analgesia.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operatingroom supplies. The video is posted here. The required parts are an operatingroomanesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps.
An anesthesia emergency occurs without warning. As the anesthesiologist, it’s your job to make the correct diagnosis and act promptly to save your patient. You need the ultimate anesthesia emergency guidebook. Anesthesia practice is described as 99% boredom and 1% panic. Will you perform perfectly?
Are anesthesiologists on the verge of being replaced by a new robot? The new device being discussed is the iControl-RP anesthesia robot. THE iCONTROL-RP ANESTHESIA ROBOT On May 15, 2015, the Washington Post published a story titled, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.”
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom. You will wear a mask in the preoperative room, and that mask will remain on your face until just prior to the induction of anesthesia.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). An anesthesiologist can easily make a diagnosis of inadequate breathing if a patient is connected to a pulse oximeter.
Why should anesthesiologists be any different? A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. A private practice anesthesia group needn’t be a physician-only group. Let’s look at the issues. How does the business work?
Here’s why the three A’s are in a different order for anesthesiology: ABILITY: For an anesthesiologist seeking a high-paying job in a competitive region of the country, the most important asset is ability. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom?
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? ” In 2018, anesthesiologists consider surgeons our colleagues, and we seek and expect collegial relationships with them.
Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. In many health care systems there are no anesthesia clinics, and primary care doctors (internal medicine specialists, family practitioners, or pediatricians) do the preoperative assessments.
The only way to end the sedative effects of propofol is for an anesthesia professional to support the airway, breathing, and circulation of the patient until the drug effects of propofol wear off in time. Anesthesiologists can manage the airway of a patient over-sedated with a benzodiazepine without need to administer a reversal agent.
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Anesthesia personnel will be in great demand.
SCALPEL, BOUGIE, TUBE APPROACH TO CRICOTHYROIDOTOMY This week I attended an outstanding Stanford Anesthesia Grand Rounds delivered by Drs. The lecture reviewed the literature regarding CICO events, and concluded that performing a surgical airway through the cricoid membrane is an essential skill for anesthesiologists.
There are hundreds of anesthesia textbooks, but which current books are the gold standards for anesthesia knowledge? Digital access to all this written expertise can be at your fingertips anywhere, including in the operatingroom suite. Cote’s book has been the bible for pediatric anesthesiologists for nearly fifty years.
In the operatingroom, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Let’s look at the anesthesia literature to learn what has been described about this problem. Her blood pressure is 150/90 on admission.
In this blog post, we’ll provide an insider’s perspective on a CRNA’s exciting and rewarding career by highlighting their daily responsibilities, how they overcome challenges, and their tremendous impact on patient care and the health field. To begin, it’s essential to understand the role of a CRNA.
The February 2020 edition of Anesthesiology , our specialty’s preeminent journal, published an article on robotic anesthesia. 1 The accompanying editorial by Dr. Thomas Hemmerling was titled “Robots Will Perform Anesthesia in the Near Future. ” robotic) anesthesia is at least as good as the best human anesthesia.
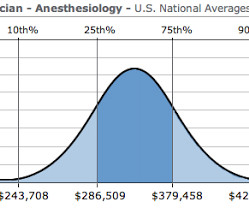
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
Medicare for All would decimate the specialty of physician anesthesiologists in America. My aim is to inform my readers, both anesthesia professionals and laypersons, that if Medicare for All becomes reality, there will be a dire consequence regarding anesthesia staffing and services to patients. of insured rates.
Photo by Magali Gauthier/The Almanac Between his time in the operatingroom, teaching, and raising his three sons, Atherton resident Dr. Rick Novak has found time to write two novels. The post DOCTOR BY DAY, SCI-FI WRITER BY NIGHT appeared first on The anesthesia consultant.
In the anesthesia world that book is now available, and it’s called Practical Anesthetic Management—The Art of Anesthesiology, authored by C. link] Their book contains a series of chapters designed to teach the anesthesia professional how to perform our craft at a higher level. Philip Larson and Richard Jaffe.
I’m an anesthesiologist, and I like to tell stories. If you wonder how much the anesthesia scene has changed significantly over the past four decades, check out this narrative: In 1986 I was in my second and final year of anesthesia residency training at Stanford, and I was looking for a job. This one is true. I was excited.
When a patient decompensates emergently at a freestanding ambulatory surgery center or in an operatingroom at a doctor’s office, the facility will call for an ambulance staffed with EMT personnel. Pulmonary edema fluid filled her lungs and filled the hoses of the anesthesia machine.
The combination of autism and anesthesia requires careful planning. The parents/guardians and the anesthesia team need to be actively involved with forming the preoperative plan for uncooperative patients. It’s not infrequent that autistic patients need surgery and anesthesia. Anesthetizing uncooperative patients is difficult.
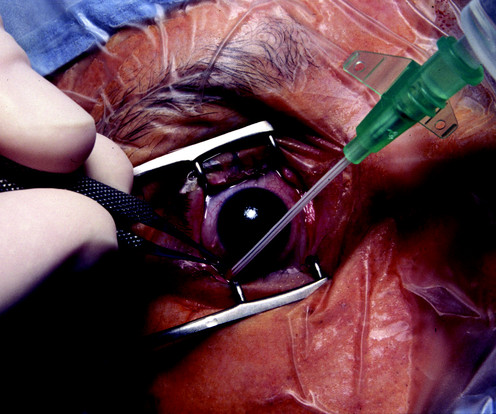
You’re are an experienced practitioner, but not a pediatric anesthesia specialist. One is how to safely perform the open-eye, full stomach anesthetic, and the other is the performance of pediatric anesthesia by non-pediatric anesthesia specialists. The second issue in this case is that you’re not a pediatric anesthesiologist.
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. In an operatingroom, the circulating nurse’s job is analogous to that of a court reporter/stenographer.
Let’s discuss an elephant in the room of operatingroomanesthesia–the association between peripheral nerve blocks and nerve injury. The use of peripheral nerve blocks has crescendoed in anesthesia practice, stimulated by the use of ultrasound-guided visualization of nerves. Liu SS, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content