This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The CSFA is not just a passive participant in the operatingroom; they are an active collaborator who anticipates the surgeons needs, manages surgical instruments, and assists with critical tasks such as suturing, tissue manipulation, and hemostasis (control of bleeding). Ensuring proper wound care and dressing application.
Moreover, these unrecognized or underrecognized secondary diagnoses reduce operatingroom efficiency by leading to cause delays and cancellations. A general truth is that surgeons prefer operating, primary care clinicians prefer managing chronic medical conditions, and anesthesiologists prefer being in the operatingroom.
Hospital surgical support encompasses a wide range of specialized services designed to assist surgeons, anesthesiologists, and nurses in performing successful surgical procedures. Prevents surgical site infections (SSIs) , a leading cause of post-operative complications. What Is Hospital Surgical Support? Why Is It Important?
Who is the Captain of the Ship in the operatingroom, the surgeon or the anesthesiologist? The Captain of the Ship doctrine was a 20 th century legal doctrine which held that, in an operatingroom, the surgeon was “liable for all actions conducted in the course of the operation.”
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists.
Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. In the control group of this study, each anesthesiologist would use a traditional ultrasound screen to visualize the artery. This was an important study, and important information.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. They also estimate 5,200 anesthesia professionals entered the workforce from training programs in 2023: 1,900 anesthesiologists, 3,000 nurse anesthetists, and 300 anesthesiologist assistants.
A doctor or a nurse? On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring., Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom.
What qualities define an outstanding anesthesiologist? Some were academic professors, some were trainees at a university, and some were community anesthesiologists either in my group or in other anesthesia companies. Rather, I’m choosing to list the qualities I’ve witnessed that make physician anesthesiologists stand out as leaders.
The Realizing Improved Patient Care through Human-Centered Design in the OperatingRoom (RIPCHD.OR) learning lab uses a socio-technical approach incorporating human factors engineering and evidence-based design principles to create an optimal ergonomically sound operatingroom that results in improved patient and staff safety.
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade.
At one New York medical center, intense clinical demands and provider fatigue have inspired one anesthesiologist to push the boundaries of clinical medicine. Dr. Mac “McGrath” Millerstein, a cardiothoracic anesthesiologist, has intubated countless patients with COVID over the last several weeks.
You utilize the current multimodal strategies for operatingroom anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% Neurosurgeons have taken him to the operatingroom to drain the hematoma and decompress the spinal column. He’s right. What happened?
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. David Gaba, Steven Howard, and Sara Goldhaber-Fiebert.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operatingroom supplies. The required parts are an operatingroom anesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps. The video is posted here.
Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Most surgeons’ comprehension of what anesthesiologists are doing is limited. The patient must wake up (when the surgery is over).
Without a doubt, the operatingroom (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. While the increased number of providers requires a higher level of supervision, the added availability of another physician to work with OR nursing enhances efficiency.
When you enter the healthcare facility, a nurse will question you regarding virus symptoms, and will screen you by taking your temperature. The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom.
Peter, MN – Physician on FIRE , an anesthesiologist and financial blogger , recently hit the magical goal of Financial Independence and Retire Early (FIRE) in his mid 40s. Once he achieved ‘FIRE status’ JACHO and hospital administration determined he was too much of a fire risk to be in the operatingroom.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). It’s also not uncommon for the patient to be breathing room air during transport.
Why should anesthesiologists be any different? In many private practice anesthesia groups, physician anesthesiologists supervise multiple nurse anesthetists in multiple operatingrooms. Physician anesthesiologists pay their nurse anesthetists as employees as well as their other expenses, and then divide the profit.
Certified Registered Nurse Anesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. With this information in mind, CRNAs collaborate with surgeons, nurses, and other healthcare professionals to develop personalized anesthesia plans to meet the specific needs of each patient.
Here’s why the three A’s are in a different order for anesthesiology: ABILITY: For an anesthesiologist seeking a high-paying job in a competitive region of the country, the most important asset is ability. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom?
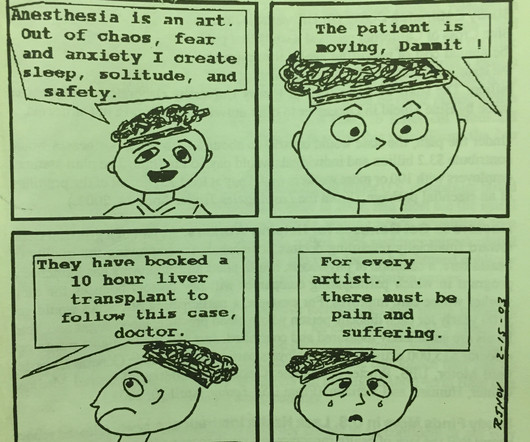
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. ” In 2018, anesthesiologists consider surgeons our colleagues, and we seek and expect collegial relationships with them. Do anesthesiologists have surgeries which last 10 hours?
Items 1 – 5 are discussed as follows: Non-anesthesiologists can reverse the effects of remimazolam with flumazenil if they overdose a patient, but this advantage is less important for anesthesia professionals. Anesthesiologists can manage the airway of a patient over-sedated with a benzodiazepine without need to administer a reversal agent.
Almost every anesthesiologist in America has experience with surgery using the da Vinci robot system. The da Vinci surgeon sits at a console in the corner of the operatingroom, with his back to the patient and his face in a 3-D viewer, which gives a high-definition, magnified view of the surgical site.
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. With an EHR it takes at least 5 clicks to chart “atropine 0.4 on the atropine line.
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). A generation ago an anesthesiologist started a case and finished that case.
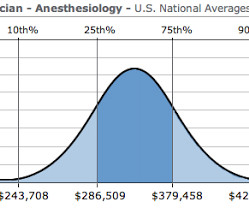
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
The key is finding the balance between optimizing operatingroom utilization and maintaining staff well-being. This unpredictability leads to a constantly changing schedule, which can result in either underutilized or overbooked operatingrooms.
Medicare for All would decimate the specialty of physician anesthesiologists in America. The Medicare pay rate for anesthesiologists is a mere fraction of the current insurance pay rate. If a physician anesthesiologist is forced to take a pay cut to 35%-45% of their previous income, they will be upset too. of insured rates.
He is verbal with his mother, but refuses to interact with the anesthesia or nursing personnel. The two hospital guards and the mother donned white operatingroom coveralls. Once the patient became sedated (2-4 minutes later), the mother was escorted from the room and the anesthesiologist started an IV in the patient’s arm.
Dawn Bent, DNP, MSN, CRNA , didn’t choose to be a nurse anesthetist as much as the profession chose her. She was working as an ICU nurse for eight years when one of the anesthesiologists that she worked with told her: “I think you would be a great nurse anesthetist.”
Dr. Jerome Adams, the Surgeon General of the United States, an anesthesiologist himself, and a professional I have tremendous respect for, tweeted this advice on February 29 th , 2020: “Seriously people- STOP BUYING MASKS! I’m talking about the looser version commonly worn in operatingrooms.
When a patient decompensates emergently at a freestanding ambulatory surgery center or in an operatingroom at a doctor’s office, the facility will call for an ambulance staffed with EMT personnel. The surgery was done in a small community hospital where there was no ICU, blood bank, or emergency room.
The second issue in this case is that you’re not a pediatric anesthesiologist. A children’s hospital or a university hospital will have a team of pediatric anesthesiologists with specialized training on call for emergencies. In my opinion, neonates and younger infants need anesthesiologists with specialized pediatric training.
You’ll become rich, and America’s doctors, nurses, and patients will bow to your achievement. Alas, doctors and nurses serve as data-entry technicians for the EPIC system of billing. EPIC is a poor system for doctors and nurses working in a hospital. If you’re a rising software engineer looking for a Holy Grail, this is it.
I’m an anesthesiologist, and my job is to keep people alive. Before her surgery, Alexandra reclined awake on the operatingroom table. Her eyes were closed, and she was unaware I’d entered the room. You can request more morphine, and the nurse in the recovery room will give it to you.” “Yes.
Lauren] debriefed me on how the days would go, the logistics of the surgeries — two operatingrooms were run simultaneously, and I had to monitor both rooms at once. “[They] personally asked me if I’d be interested in attending,” said Devon. “As As this was a unique opportunity that does not come along often, I said yes!
My career has bridged clinics, operatingrooms, intensive care units, emergency rooms, and helicopter trauma medicine. In the 21 st century operatingroom practice of anesthesiology, we typically have ten minutes to talk to a patient prior to rendering them unconscious. I’ve practiced in four different decades.
This is the group of scrub techs and nurses that I worked with for the week. I had to find it, or find someone who could help me find it, before I could bring it back to the room. No one in the room knew me, and I desperately wanted to do well and demonstrate that I really was a competent OR nurse.
Each operatingroom anesthesia location is the epicenter of computerized medical record-keeping machines, computerized Pyxis-style drug storage systems, computerized labeling machines, and bar-code reading billing machines. Sugammadex is the single most important new medication in the toolbox of the 21 st -century anesthesiologist.
The teams included plastic surgeons, anesthesiologists, pediatricians, and nurses experienced in the care of cleft palate reconstructions. Because there were dozens of cases to be done, the anesthesia attending and the anesthesia resident each did their cases alone and independently, in adjoining operatingrooms.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content