This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. Imagine this: It’s the year 2034.
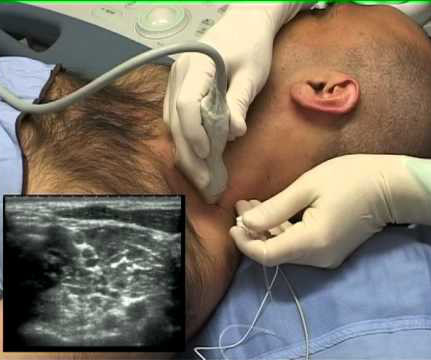
Wearing smart glasses improved the anesthesiologist’s first-attempt success rate, and reduced the procedure time and complication rates. In the control group of this study, each anesthesiologist would use a traditional ultrasound screen to visualize the artery. This was an important study, and important information.
In recent years, engineers have developed closed-loop AI machines that can administer appropriate doses of anesthetics without human input , as described in The Washington Post article, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Thus, we might ask, ‘What happens to the operator/clinician involved?’
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring., Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). Are CRNAs and anesthesiologists equals?
What qualities define an outstanding anesthesiologist? A bell-shaped curve exists for the abilities of anesthesia doctors as well. I’ve been practicing anesthesia since the mid 1980s. I’ve met and worked alongside hundreds of anesthesia colleagues from all corners of the globe. This can be a vain conceit. Be prepared.
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade. Why Did Take Me So Long To Wake From GeneralAnesthesia?
Anesthesia emergencies are anxiety-producing for both experienced and inexperienced anesthesiologists, but experienced doctors are more likely to know exactly what to do and what not to do. Perioperative” means “the time around an operation”—specifically the preoperative, postoperative, and intraoperative times.
Will Gawande change the future for anesthesiologists? Let’s look at these three proposed Gawande changes, and how they affect the future for anesthesiologists: Taking out the trash. This proposed elimination of wasteful spending would decrease the demand for anesthesia professionals.
At one New York medical center, intense clinical demands and provider fatigue have inspired one anesthesiologist to push the boundaries of clinical medicine. Dr. Mac “McGrath” Millerstein, a cardiothoracic anesthesiologist, has intubated countless patients with COVID over the last several weeks.
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% How can an anesthesiologist make such an error? He’s right. What happened?
Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Most surgeons’ comprehension of what anesthesiologists are doing is limited. The patient must wake up (when the surgery is over).
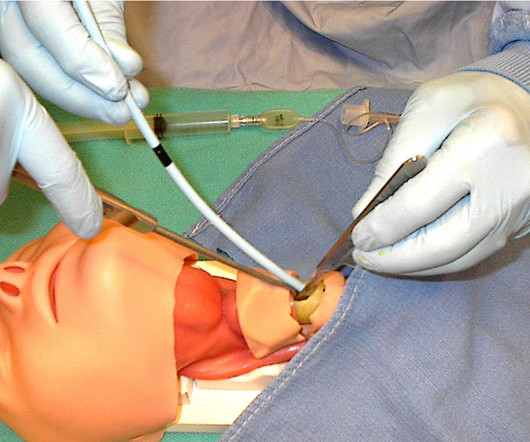
Miller 2 Direct Laryngoscope Video Laryngoscope When it’s time to insert an endotracheal tube, for decades anesthesiologists have utilized a direct laryngoscope. Direct laryngoscopy (DL) is a difficult skill to acquire, but all anesthesiologists become masters of it. Enter the video camera, which changed surgical practice.
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. Both were published in the journal Anesthesia and Analgesia.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). An anesthesiologist can easily make a diagnosis of inadequate breathing if a patient is connected to a pulse oximeter.
An anesthesia emergency occurs without warning. As the anesthesiologist, it’s your job to make the correct diagnosis and act promptly to save your patient. You need the ultimate anesthesia emergency guidebook. Anesthesia practice is described as 99% boredom and 1% panic.
Some health care systems run preoperative anesthesia clinics, where anesthesia professionals evaluate these patients prior to surgery. In many health care systems there are no anesthesia clinics, and primary care doctors (internal medicine specialists, family practitioners, or pediatricians) do the preoperative assessments.
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operatingroom. You will wear a mask in the preoperative room, and that mask will remain on your face until just prior to the induction of anesthesia.
The two hospital guards and the mother donned white operatingroom coveralls. At the mother’s consent, the guards laid the patient down on the hospital gurney, held him there, and the surgical team and the guards pushed the gurney down the hallway to the operatingroom (a significant distance of approximately 100 yards).
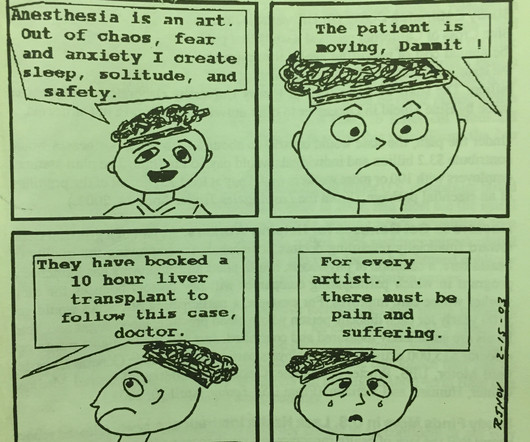
THIS ORIGINAL ANESTHESIA CARTOON WAS PUBLISHED IN THE CALIFORNIA SOCIETY OF ANESTHESIOLOGISTS BULLETIN, VOLUME 52, NUMBER 2, APRIL-JUNE 2003. IS ANESTHESIA AN ART OR A SCIENCE? ” In 2018, anesthesiologists consider surgeons our colleagues, and we seek and expect collegial relationships with them.
Why should anesthesiologists be any different? A private practice single-specialty anesthesia group will usually provide anesthesia for similarly self-employed surgeons who are in private practice. A private practice anesthesia group needn’t be a physician-only group. Let’s look at the issues. Employees of whom?
Here’s why the three A’s are in a different order for anesthesiology: ABILITY: For an anesthesiologist seeking a high-paying job in a competitive region of the country, the most important asset is ability. Do you think patients want a friendly anesthesiologist who is all thumbs in the operatingroom?
How will astronauts conduct generalanesthesia and surgery in outer space? Is an anesthesiologist required on board? Protocols regarding how to accomplish anesthesia in outer space exist in the medical literature. Is a surgeon required on board?
A non-anesthesia-professional can administer remimazolam, whereas an anesthesia professional/airway expert must administer and monitor propofol administration. Anesthesiologists can manage the airway of a patient over-sedated with a benzodiazepine without need to administer a reversal agent. Are these advantages important?
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). A generation ago an anesthesiologist started a case and finished that case.
Digital access to all this written expertise can be at your fingertips anywhere, including in the operatingroom suite. The Anesthesia Consultant’s 2022 List of the Top Anesthesia Books includes: Miller’s Anesthesia , 9th edition, 2019, Editor-in-Chief Michael Gropper.
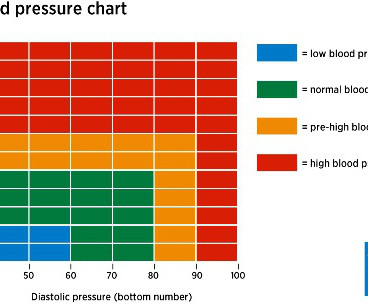
In the operatingroom, you induce anesthesia with your standard recipe of 2 mg of midazolam, 100 mcg of fentanyl, 200 mg of propofol, and 40 mg of rocuronium, and intubate the trachea. Predictors of hypotension after induction of generalanesthesia Anesth Analg. Her blood pressure is 150/90 on admission.
One of the changes our profession has gone through is an ever-increasing demand to multitask, be it by running more than one operatingroom, or by simultaneously performing administrative or teaching tasks. How will we do anesthesia in the future? Can I get a propofol, remifentanil-based anesthesia?
The lecture reviewed the literature regarding CICO events, and concluded that performing a surgical airway through the cricoid membrane is an essential skill for anesthesiologists. Most anesthesia professionals have never cut into a patient’s neck, but we must own this skill if the necessity arises.
I’m an anesthesiologist, and I like to tell stories. If you wonder how much the anesthesia scene has changed significantly over the past four decades, check out this narrative: In 1986 I was in my second and final year of anesthesia residency training at Stanford, and I was looking for a job. This one is true. I was excited.
Are anesthesiologists on the verge of being replaced by a new robot? The new device being discussed is the iControl-RP anesthesia robot. THE iCONTROL-RP ANESTHESIA ROBOT On May 15, 2015, the Washington Post published a story titled, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” In a word, “No.”
When a patient decompensates emergently at a freestanding ambulatory surgery center or in an operatingroom at a doctor’s office, the facility will call for an ambulance staffed with EMT personnel. Why did an anesthesiologist travel with each patient? The patient was discharged the following day without further complication.
Between them, Larson and Jaffe have taught hundreds of anesthesia residents the finer points of clinical care. Now, because of this book, readers can find on the printed page what the authors taught in the preoperative forum, in the operatingroom, and in the post-anesthesia recovery room. Together, Drs.
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. In an operatingroom, the circulating nurse’s job is analogous to that of a court reporter/stenographer.
The second issue in this case is that you’re not a pediatric anesthesiologist. A children’s hospital or a university hospital will have a team of pediatric anesthesiologists with specialized training on call for emergencies. It’s common for generalanesthesia practitioners to cover many or all specialties when they’re on call.
Medicare for All would decimate the specialty of physician anesthesiologists in America. My aim is to inform my readers, both anesthesia professionals and laypersons, that if Medicare for All becomes reality, there will be a dire consequence regarding anesthesia staffing and services to patients. of insured rates.
Let’s discuss an elephant in the room of operatingroomanesthesia–the association between peripheral nerve blocks and nerve injury. The use of peripheral nerve blocks has crescendoed in anesthesia practice, stimulated by the use of ultrasound-guided visualization of nerves. Of course not.
Almost every anesthesiologist in America has experience with surgery using the da Vinci robot system. The da Vinci surgeon sits at a console in the corner of the operatingroom, with his back to the patient and his face in a 3-D viewer, which gives a high-definition, magnified view of the surgical site.
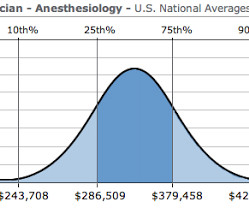
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
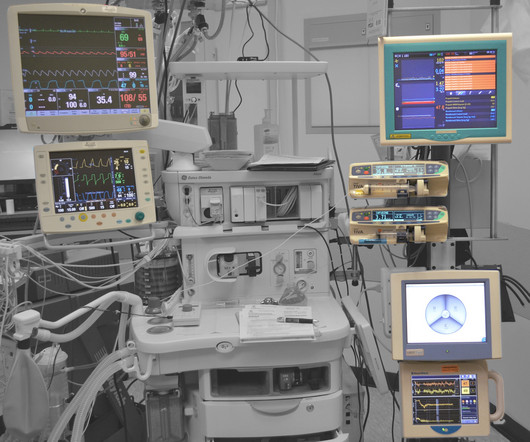
How can it be that generalanesthesia has ceased to evolve? Anesthesia in 2018 is markedly different from anesthesia in the 1990s. Most of the drugs in use haven’t changed, but current-day anesthesia providers practice in a cockpit surrounded by computers. Why Did Take Me So Long To Wake From GeneralAnesthesia?
The 2023 American Society of Anesthesiologists Practice Guidelines for Monitoring and Antagonism of Neuromuscular Blockade were published last month.The paper is backed by strong science, and references an exhaustive list of no less than 277 previous publications on the topic, including this review. A 2010 survey documented that 9.4%
My career has bridged clinics, operatingrooms, intensive care units, emergency rooms, and helicopter trauma medicine. In the 21 st century operatingroom practice of anesthesiology, we typically have ten minutes to talk to a patient prior to rendering them unconscious. What Are the Common Anesthesia Medications?
A QUANTITATIVE NEUROMUSCULAR MONITOR How do anesthesiologists monitor the degree to which a patient’s muscles are pharmaceutically paralyzed during an anesthetic? Should the American Society of Anesthesiologists (ASA) add QUANTITATIVE neuromuscular monitoring as a standard of care? Will I Have a Breathing Tube During Anesthesia?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content