This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Who is the Captain of the Ship in the operating room, the surgeon or the anesthesiologist? The operating room team today consists of multiple professionals working in collaboration, including the surgeon, the scrub tech, the circulating nurse, and the anesthesia MD or CRNA.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered Nurse Anesthetists). A doctor or a nurse?
In a professional labor market such as anesthesia providers, the supply of qualified clinicians cannot increase fast enough to ease the pressures resulting from a markedly increasing demand. Specific trends have led to the anesthesia workforce supply–demand relationship.
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The University of Michigan paper stated, “this study primarily analyzed physician-CRNA teams, the dominant practice model in US anesthesiology.”
What’s the difference between a physician anesthesiologist and a nurse anesthetist? After the first 3 – 4 years in the workforce, either one can master the manual skills of anesthesia. So what really is the difference between a physician anesthesiologist and a nurse anesthetist? The answer: internal medicine.
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade. Why Did Take Me So Long To Wake From GeneralAnesthesia?
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring., To the contrary, in our practice we physician anesthesiologists start the IVs ourselves.
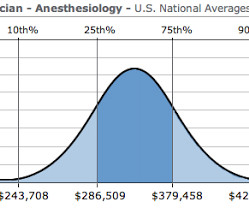
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
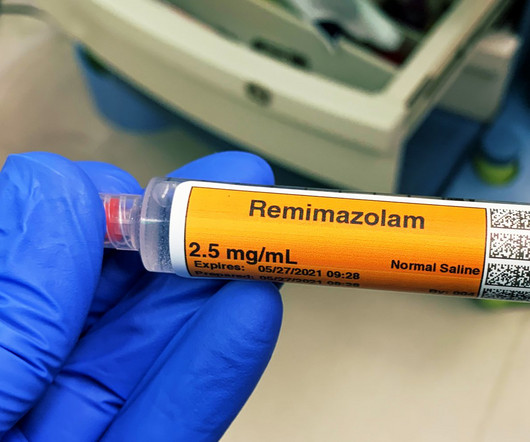
A non-anesthesia-professional can administer remimazolam, whereas an anesthesia professional/airway expert must administer and monitor propofol administration. Anesthesiologists can manage the airway of a patient over-sedated with a benzodiazepine without need to administer a reversal agent. Total intravenous anesthesia (TIVA).
I wish I’d had the foresight and the money ten years ago to invest in a factory that produced generic anesthetic drugs. The cooperation between surgeons, anesthesiologists, and internal medicine specialists to develop the protocols has been outstanding, the standardized checklist care has been well accepted, and patients are benefiting.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The anesthesiologist meets the patient prior to the surgery, reviews the chart, and examines the patient.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesiaanesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). Anesthesiologists are vigilant during extubation.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operating room. Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient.
During the dayshift, working alone is seldom an issue for any anesthesiologist. A typical hospital will have dozens of other anesthesia providers working in the same building. Within seconds or minutes, any anesthesiologist can be assisted or bailed out by a colleague. There are multiple different models of anesthesia care.
Today I read a thoughtful and well-written essay in Anesthesiology News titled, Anesthesiologists-The Utility Players of the Medical Field written by anesthesiologist David Stinson MD from my native state of Minnesota. To me, the appropriate headline should read, “Anesthesiologists—the Most Valuable Players of the Medical Team.”
You’re an anesthesiologist. I’d like to focus on one specific aspect of this important study: anesthesiologists need to lose their reluctance to cut a surgical airway into a patient’s neck in a “can’t intubate, can’t oxygenate” airway emergency. Case 5: “The anesthesiologist asked the surgeon to perform an emergency cricothyrotomy.
This is what the anesthesia experience is like for most patients: You show up for surgery, and some anesthesia professional you’ve never met or talked to appears 10 minutes before you are to be wheeled into the operating room. The anesthesia professional might be an MD, a CRNA, or both a MD and a CRNA might be involved.
Is it feasible that CHATGPT, this decades artificial intelligence wunderkind, can equal or better a physician anesthesiologist? I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. Why Did Take Me So Long To Wake From GeneralAnesthesia?
A board-certified physician anesthesiologist is therefore validated as an expert in all areas of perioperative medicine. Most anesthetics are conducted by physician anesthesiologists. In this model, an MD anesthesiologist supervises up to four CRNAs who work in up to four different operating rooms simultaneously.
These three words make any anesthesiologist cringe. If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The anesthesiologist decided to extubate the trachea.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content