This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
It’s a path that demands not only clinical excellence but also a significant shift in roles—from direct patientcare in a high-intensity setting to the precision and autonomy of anesthesia. Understanding the Shift The transition from ICU to operatingroom (OR) involves a fundamental change in responsibilities.
The Realizing Improved PatientCare through Human-Centered Design in the OperatingRoom (RIPCHD.OR) learning lab uses a socio-technical approach incorporating human factors engineering and evidence-based design principles to create an optimal ergonomically sound operatingroom that results in improved patient and staff safety.
OperatingRoom (OR) nurses, also known as perioperative nurses, play an essential role in surgeries. They are responsible for maintaining a sterile environment, assisting surgeons, and ensuring patient safety throughout the surgical process. The post What is an OR Nurse and What Do They Do in the OperatingRoom?
Anesthesiology residents play an important role in the operatingroom (OR), assisting with patientcare while also undergoing rigorous training to become skilled anesthesiologists. Their responsibilities encompass a range of tasks, from preoperative evaluations to the administration of anesthesia and postoperative care.
Post-AnesthesiaCare Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operatingroom and continues until they are stable enough to recover at home or in a hospital room. Their role in maintaining the flow of operations cannot be overstated.
The February 2020 edition of Anesthesiology , our specialty’s preeminent journal, published an article on robotic anesthesia. 1 The accompanying editorial by Dr. Thomas Hemmerling was titled “Robots Will Perform Anesthesia in the Near Future. ” robotic) anesthesia is at least as good as the best human anesthesia.
When you think of the operatingroom (OR), what comes to mind? I first learned how to scrub – setting up the instruments and handing them to the surgeon during the procedure – and then I moved into circulating, a more typical RN role of providing direct patientcare before, during and after the procedure.
Without a doubt, the operatingroom (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. to improve the bottom line, changes to the existing anesthesia staffing model may help. link] The Three Anesthesia Staffing Models: The optimal hospital staffing model should: 1.
The operatingroom (OR) is a team based unit where patients undergo surgical procedures. One of the best parts about the OR is taking care of one patient at a time. Surgical nursing is unlike any other nursing specialty or unit.
In the anesthesia world that book is now available, and it’s called Practical Anesthetic Management—The Art of Anesthesiology, authored by C. link] Their book contains a series of chapters designed to teach the anesthesia professional how to perform our craft at a higher level. Philip Larson and Richard Jaffe.
In this blog post, we’ll provide an insider’s perspective on a CRNA’s exciting and rewarding career by highlighting their daily responsibilities, how they overcome challenges, and their tremendous impact on patientcare and the health field. To begin, it’s essential to understand the role of a CRNA.
The inside of the healthcare facility will be cleaned prior to any patientcare, and will be recleaned after each patient leaves an operatingroom. Healthcare workers take respiratory precautions with all patients as if that patient was COVID positive, whether the COVID test result has come back yet or not.
Ngin studied to become a nurse at Villanova University near Philadelphia and planned to become a pediatric critical care nurse practitioner. Part of her pediatric critical care transport training involved performing advanced airway management in the operatingroom.
Additionally, these providers (like assistants) perform preoperative and postoperative duties that are essential to patientcare. If you’re wondering how your hospital or surgery center could benefit from the integration of these professionals, here are three ways that they improve patient outcomes.
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. The economics don’t add up, and have nothing to do with patientcare.
Clinic doctors see multiple patients per day, perhaps 4-8 patients per day for psychiatrists, and up to 30 patients or more for some specialists such as allergists. Their job description includes teaching younger doctors and mentoring younger doctors in patientcare. Housestaff back-up.
In the ever-evolving landscape of healthcare, the integration of data-driven practices is heralding a new era of efficiency and patientcare. Since then, she has spearheaded initiatives in the optimization of OperatingRoom (OR) management.
ASCs’ efficiency, lower costs, and high-quality patientcare often allow them to earn higher margins than traditional surgical settings like hospital ORs or hospital outpatient departments (HOPDs). With rising anesthesia costs and stagnating reimbursements, ASCs’ margins are thinner than they were even five years ago.
The challenges for operatingroom (OR) managers are universal: improving surgical workflow efficiency while providing high-quality, reliable, safe patientcare. They monitor from the time the patient arrives at the hospital for surgery until the time that they have a nurse assigned to them.
View Critical care RN Sample Resume 7. OperatingRoom, Perioperative or Surgical Services Resume Example OperatingRoom Registered Nurses (OR RNs) can be named by various nursing job titles including surgical services registered nurses and/or perioperative registered nurses.
Patient safety should be at the top of everyone’s priority list, and when everything is viewed through that lens, then we realize that every department assisting surgical services adds value and should be given the proper consideration for how they affect our patient outcomes. But instead, let’s look at SPD.
Anesthesia is a hands-on specialty. Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient.
Anesthesiologists aren’t well known to most patients, but these specialty doctors have certain traits in common. Anesthesiologists are likely to have: A preference for being in an operatingroom rather than in a clinic. Most of the time an anesthesiologist works in the operatingroom. They have to be.
He writes, “Our specialty, anesthesia, has suffered an identity crisis for decades. In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operatingroom. Five minutes later, the patient had a cardiac arrest. Hold your heads high.
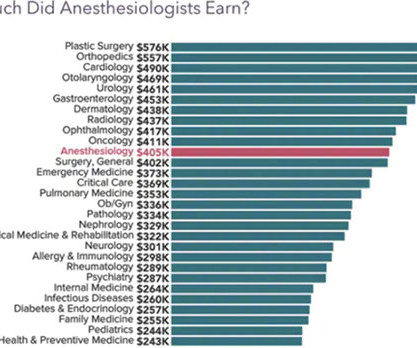
Only 12 percent of the hospitals studied received net profits of more than $1,000 per patient when payments from insurers, government, and the patients themselves were included. 2 An anesthesia group’s success is closely tied to the fate of their hospital. shifts at an ASC, and anesthesia groups covet such work.
It’s within the resources of every anesthesia residency program to provide Mock Oral Exams for their trainees. Faculty Member A) begins by asking 10 minutes of questions dealing with preoperative anesthesia issues, followed by 15 minutes of questions about intraoperative issues by the second examiner (e.g. Monitoring. Why or why not?
i²medi and Picis proudly announced the successful implementation of the Picis OR MANAGER®, a comprehensive operatingroom management system, into one of Mexico’s major hospital networks. This achievement signifies a substantial advancement in surgical planning, operating theater optimization, and overall hospital productivity.
A review of the medical literature on Pubmed shows no peer-reviewed studies or data that surgery centers provide less safe care than hospitals. Surgery and anesthesia are never 100% safe, no matter where procedures are done. The legal term for this is that physicians must adhere to the “standard of care.” There are always risks.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
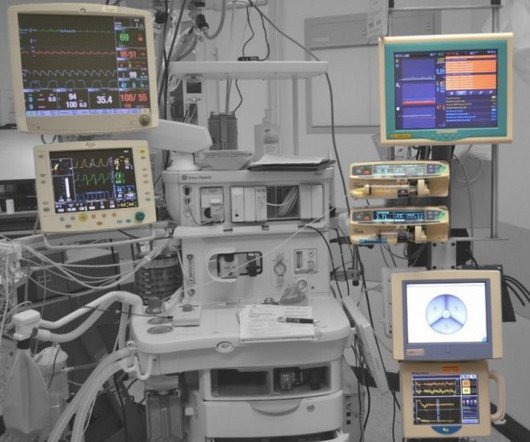
Why Data Across the Surgical Continuum Matters Integrated operatingrooms have reshaped surgery in the past decade, providing amongst other benefits, enhanced communication, shortened surgical times, reduced patient cancellations, real-time access to patient information and advanced imaging, as well as maximum use of operatingrooms.
Real-Time Monitoring for Enhanced Patient Safety: AI algorithms can act as a vigilant “second set of eyes”across all surgeries, continuously monitoring patient vital signs, anesthesia levels, and other critical parameters.
Last-minute changes in the patient’s condition, such as fluctuations in blood pressure or an allergic reaction to anesthesia, may also cause delays as the team aims to stabilize the patient 1. The availability of operatingrooms plays a critical role in surgery start times. References 1.Meneveau,
by PennLive.com Patients undergoing surgery or procedures requiring anesthesia are safe when cared for by a physician anesthesiologist, a certified registered nurse anesthetist (CRNA), or both. Published: Jan. 12, 2025, 10:00 a.m.
At Caresyntax, we are leveraging the capabilities of artificial intelligence (AI) to provide a comprehensive safety net that reinforces patient health and supports surgical staff both inside and out of the operatingroom (OR).
Patient access to surgical care is expected to be impacted by several factors, including the growing use of digital and virtual health tools, increasing focus on outpatient care, shifting system design, the closing of rural hospitals, and continued advancements in AI in patientcare.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content