This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% 300 mg of morphine, and a light general anesthetic using 1-1.5% 300 mg of morphine, and a light general anesthetic using 1-1.5%
Shortly after, the spinal anesthetic wore off and the patient was quickly placed under generalanesthesia. Apart from paralysis as a result of a spinal epidural hematoma, the procedure was a resounding success. Millerstein ducked, administered intramuscular ketamine to Dr. Annuloplasty, and a major crisis was averted.
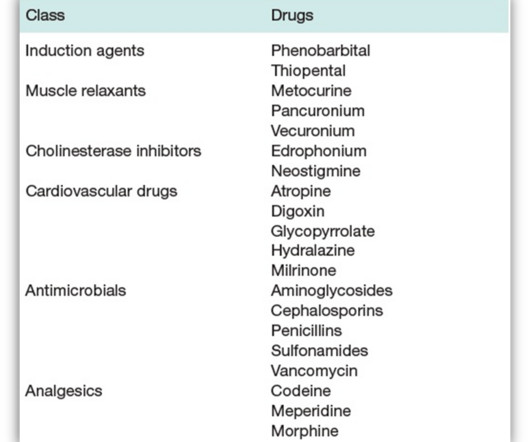
For example, anesthesia may decrease RBF by dropping CO or MAP. Sympathetic stimulation occurs secondary to surgical stress, generalanesthesia, hypoxia, hypotension, pain, severe bleeding, and strenuous exercise. What are the drugs used or encountered in anesthesia practice that significantly depend on renal elimination?
ANESTHESIA FOR CESAREAN DELIVERY FOR CARDIAC PATIENTS: • Patients with mWHO class I or II cardiac disease typically tolerate a traditional intrathecal dose of local anesthesia (eg, hyperbaric bupivacaine 10–15 mg) for cesarean delivery. Obstetric anesthesia management of the patient with cardiac disease. REVIEW ARTICLE.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. What went wrong?
The study looked at malpractice closed claims and found: 1) Outcomes remained poor in malpractice closed claims related to difficult tracheal intubation; 2) The incidence of brain damage or death at induction of anesthesia was 5.5 This training needs to be a requirement for all anesthesia professionals.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content