This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transitioning from working as an ICU nurse to becoming a Certified Registered NurseAnesthetist (CRNA) is a journey marked by immense growth but also profound challenges. ICU nurses are adept at managing complex critical care situations, which provides a solid foundation for a career in anesthesia.
What’s the difference between a physician anesthesiologist and a nurseanesthetist? There is no fork in the career path that makes a busy Certified Registered NurseAnesthetist (CRNA) automatically inferior to a medical doctor anesthesiologist in hands-on skills. The answer: internal medicine. In a way, it is.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. Non-emergency surgery may be delayed for days, weeks, or longer. Consolidation of surgery locations from understaffed rural facilities to urban/suburban hospitals and surgery centers is likely.
A nursing degree unlocks a plethora of career opportunities. With an array of jobs you can get with a nursing degree , choosing your path might seem daunting, but it doesn’t have to be. This article aims to simplify your search for nursing degree jobs , shedding light on various nursing roles.
Advanced Practice Provider Spotlight: Certified registered nurseanesthetist shares perspective on caring for diverse patients Posted April 11, 2023 by ,Penn State Health News Prolung Ngin , a certified registered nurseanesthetist (CRNA) at Penn State Health Milton S.
A doctor or a nurse? The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered NurseAnesthetists). A quote from the Medscape article read: “Adam Dachman, MD, a surgeon at the hospital, speaking for himself, said he has no problem using nurseanesthetists.
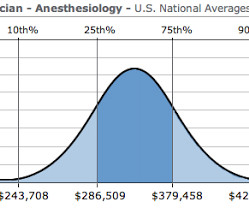
The job of a certified nurseanesthetist was listed as #11 on the Best Paying Jobs list. The median salary of nurseanesthetists was listed as $160,270, and the unemployment rate as 2.7%. Expect the demand for acceptance into physician anesthesiologist and nurseanesthetist training programs to remain high.
Certified Registered NurseAnesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. CRNAs received specialized training that is critical in surgeries and healthcare. As a critical component of a successful surgery, CRNAs are constantly assessing the patient’s vitals and pain level/comfort.
Ashley Bell, BSN, RN , has always been fascinated by the way patients are put into a state where they are unable to feel and respond to outside stimuli, and then when they awake, they have no recollection of what took place throughout the surgery.
While few administrators would consider reducing the number of surgeries (that would strangle the golden goose!) All MD In this model, (most prevalent in one-or two-room surgery centers and less common in large ambulatory surgery centers), all anesthesia care is provided by medical doctors only, specifically physician anesthesiologists.
An anesthesiologist is a medical doctor who plays a critical role in the preparation, execution, and recovery stages of surgery. Additionally, the anesthesiologist leads teams of certified registered nurseanesthetists ( CRNA s) and certified anesthesiologist assistants (CAAs).
The Anesthesia Consultant exists to increase your knowledge about anesthesia and the practice of medicine before, during, and after surgery. The other half are detailed, well-referenced articles aimed at physician anesthesiologists, nurseanesthetists, and anesthesia assistants the world over.
It’s not clear the idea has widespread traction as of yet, and the concept will always be at odds with the individual aspirations of internal medicine doctors, hospitalists, intensivists, surgeons, and certified nurseanesthetists, all who want to make their own management decisions, and all who desire to be paid for owning those decisions.
In many private practice anesthesia groups, physician anesthesiologists supervise multiple nurseanesthetists in multiple operating rooms. Physician anesthesiologists pay their nurseanesthetists as employees as well as their other expenses, and then divide the profit.
In anesthesiology residency training we learn to perform every kind of anesthetic—cardiac, trauma, brain surgery, transplant surgery, abdominal surgery, chest surgery—on every type of patient—newborns, one-hundred-year-olds, or pregnant women. What kind of cases do you want to do when you’re out of training?”
The patient must wake up (when the surgery is over). Surgeons work with physician anesthesiologists, with certified nurseanesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. The patient must wake up (when the surgery is over).
Do anesthesiologists have surgeries which last 10 hours? 12 Important Things to Know as You Near the End of Your Anesthesia Training Should You Cancel Surgery For a Blood Pressure = 178/108? Yes, we do, and that’s a long time to remain vigilant. Hibbing also happens to be the hometown of music icon Bob Dylan.
A landmark study published in Anesthesiology Dokkedal U et al, Cognitive Functioning after Surgery in Middle-aged and Elderly Danish Twins. Results from cognitive tests were compared in twins in which one sibling was exposed to surgery and the other was not. Anesthesiology. 2016 Feb;124(2):312-21 answers this question.
including pediatric open heart surgery, and pediatric surgery involving major blood loss). In 2021 a nurseanesthetist publication looked at the use of Google Glass by seven nurseanesthetists for display of the vital signs monitor , but there were no quantitative data to examine the significance of the technology.
12 Important Things to Know as You Near the End of Your Anesthesia Training Should You Cancel Surgery For a Blood Pressure = 178/108? Joining the hospital staff, Nico runs afoul of a grouchy nurseanesthetist calling himself Bobby Dylan, who plays Dylan songs twice a week in a bar called Heaven’s Door.
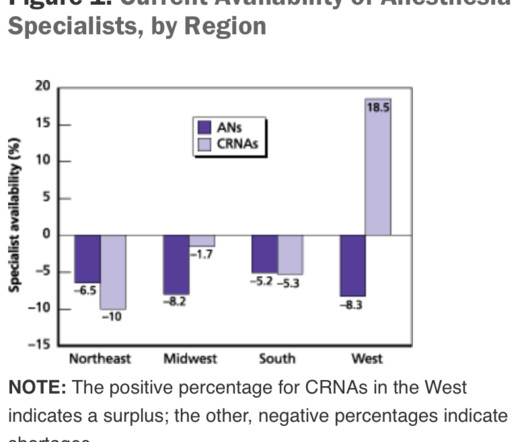
Growing shortages of anesthesiologists globally could significantly impact the availability of surgeries and other medical procedures, especially in rural and low-income areas. Similarly, a study from the UK suggests that there will be a shortage of 11,000 anesthetic staff members by 2040, preventing 8.25
Anesthetist options were limited. Before her surgery, Alexandra reclined awake on the operating room table. Can you people just get this surgery over with? You can request more morphine, and the nurse in the recovery room will give it to you.” “Yes. During the surgery you’ll have a breathing tube in your throat.
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. Nurses consistently have their backs to patients as they type, type, type data into computer terminals.
More care team anesthesia and more Certified NurseAnesthetists (CRNAs). An aging population, an increased volume of surgery, and an increased demand for anesthesia personnel. As the baby boomers age, there will be an increased number of surgeries on older, sicker patients. Anesthesia personnel will be in great demand.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). The first surgery today is a procedure devised to treat obstructive sleep apnea, a procedure called a maxillary-mandibular osteotomy. The surgery will take approximately three hours. You’ll be asleep for the entire surgery.
The good news for the future of anesthesia careers is that the number of surgeries in the United States is expected at increase as the Baby Boomers age. As stated above, the good news for the future of anesthesia careers is that the number of surgeries in the United States is expected at increase as the Baby Boomers age.
It’s not infrequent that autistic patients need surgery and anesthesia. Dental cases are common, and are frequently referred to a hospital because the typical care systems at an outpatient surgery center or a dental office are inadequate to complete a successful anesthetic. What do you do?
You have to get along well with surgeons, the nursing staff, the scrub techs, administrators, and the patients. Their patients are obtunded on arrival to the Post Anesthesia Care Unit (PACU) after surgery, and they rely on the PACU nursing staff to complete the job of anesthesia wake up. Be friendly and personable.
This likely would lead to an increased role for certified nurseanesthetists (CRNAs), and an eventual increase in the number of schools training CRNAs, but in the short term there would be no way to staff adequate numbers of anesthesia professionals.
Listening to some of its disciples, it would seem that nearly every orthopedic surgery procedure can benefit from an ultrasonic regional block for intraoperative and postoperative pain control. 12 Important Things to Know as You Near the End of Your Anesthesia Training Should You Cancel Surgery For a Blood Pressure = 178/108?
When a patient needs an epidural for surgery, the recipe of bupivicaine or lidocaine +/- narcotic is unchanged from the 1990s. Administering local anesthetic injections adjacent to major nerves grants non-narcotic pain relief to thousands of patients following orthopedic surgeries. What about regional anesthesia?
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. There were approximately 21 million surgeries per year in the United States in 2014. Anesthesiologists do not routinely read JAMA Surgery and may be quick to dismiss the findings.
12 Important Things to Know as You Near the End of Your Anesthesia Training Should You Cancel Surgery For a Blood Pressure = 178/108? Joining the hospital staff, Nico runs afoul of a grouchy nurseanesthetist calling himself Bobby Dylan, who plays Dylan songs twice a week in a bar called Heaven’s Door.
I stay with the child until the anesthetic depth has dissipated, the breathing tube is removed, and the child is awake and safe with the recovery room nurse in the Post Anesthesia Care Unit. Your reward for becoming a doctor will arrive years later, when you feel what I feel when I reunite parents with their child after surgery.
A few non-medical professionals wrote articles in magazines, newspapers, and encyclopedias to explain medical facts, diagnoses, and therapy to the lay public, but the overwhelming majority of the information was only presented to doctors and nurses in the form of medical books and journals.
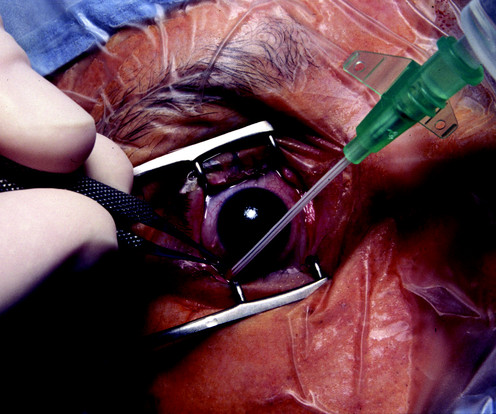
In his judgment delaying the surgery would increase the patient’s risk of loss of vision. At the conclusion of surgery, because of the full stomach, the patient is extubated awake. 12 Important Things to Know as You Near the End of Your Anesthesia Training Should You Cancel Surgery For a Blood Pressure = 178/108?
Coughing and bucking are associated with increases in blood pressure and heart rate, as well as increased intrathoracic pressure, intracranial pressure, intraocular pressure, and increased bleeding or edema in head and neck surgeries. His question prompted me to write this column. Results showed the addition of this single dose (0.5
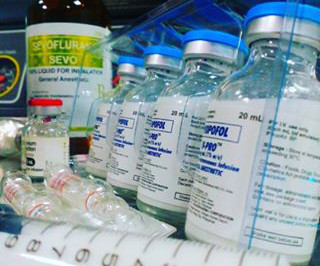
For example, in a general anesthetic for an abdominal surgery, the anesthesiologist may inject Versed into the IV as a premedication to reduce anxiety, then inject propofol into the IV to initiate sleep, and inject rocuronium into the IV to induce muscle relaxation/paralysis prior to inserting an endotracheal breathing tube.
Propofol administration requires an experienced clinician, e.g. either an anesthesiologist, a certified registered nurseanesthetist (CRNA), or an emergency medicine physician. Since midazolam (Versed) was approved in 1982, a standard anesthesia practice has included a 2 mg dose of Versed prior to surgery to calm a patient’s anxiety.
During this COVID crisis, intensive care unit and emergency room doctors and nurses in hotspots like New York City have dangerous, exhausting jobs keeping coronavirus patients alive. A minority of doctors and nurses are saddled with these dangerous around-the-clock jobs battling the disease in ICUs and ERs.
No, it’s not the nurseanesthetists, nor the stress of covering surgeries in the middle of the night, nor the stress of saving patients who are trying to die in front of our eyes during acute care emergencies. In their operating room role they more resemble the niche of a surgeon than that of an anesthetist.
Who is responsible for your safety before, during, and after your surgery? Will it be a nurse or will it be a physician? The word “perioperative” means “around the time of surgery.” It’s officially defined as the 30-day time period following surgery. Note this data was for inpatient surgeries. No, they are not.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The anesthesiologist meets the patient prior to the surgery, reviews the chart, and examines the patient.
“Why do I have to stop eating and drinking prior to surgery?” This is a common question I hear from my patients—they’re puzzled by the connection between going to sleep and stopping eating prior to surgery. It’s vital that your stomach is empty prior to elective surgery and anesthesia.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content