This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transitioning from working as an ICU nurse to becoming a Certified Registered NurseAnesthetist (CRNA) is a journey marked by immense growth but also profound challenges. Understanding the Shift The transition from ICU to operating room (OR) involves a fundamental change in responsibilities.
Finally becoming a Certified Registered NurseAnesthetist (CRNA) comes with a lot of excitement—and responsibility. That’s why we’re excited to announce the Society of Future NurseAnesthetists’ new partnership with NSO , offering a special New Graduate Discount on professional liability insurance.
What’s the difference between a physician anesthesiologist and a nurseanesthetist? There is no fork in the career path that makes a busy Certified Registered NurseAnesthetist (CRNA) automatically inferior to a medical doctor anesthesiologist in hands-on skills. The answer: internal medicine.
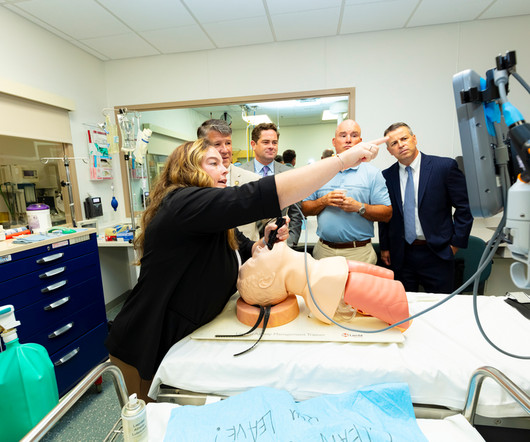
Seeing is believing and several northeastern Pennsylvania lawmakers and staff got a firsthand look at just a few of the intensive education and training programs that students must master to become certified registered nurseanesthetists (CRNAs). Eddie Day Pashinski (D-Luzerne) to visit and check out the university’s simulation labs.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. The Center for Anesthesia Workforce Studies estimates that current clinically active anesthesia professionals are made up of 43,500 anesthesiologists, 50,000 nurseanesthetists, and 3,200 anesthesiologist assistants.
Pre-operative anxiety , the psychological distress which patients experience that is provoked by concerns related to their surgical and anesthetic care, 1 is estimated to affect up to 75% of children 2 and 80% of adult patients. 3,4 It has been linked to multiple intra-operative and post-operative complications (e.g.,
In the smart glasses group, the ultrasound machine was located behind the operator, and the smart glasses were paired with the ultrasound machine. Would the addition of smart glasses for routine monitoring be an overdose of technology in the operating room cockpit? The physician medical literature has not studied the issue.
Advanced Practice Provider Spotlight: Certified registered nurseanesthetist shares perspective on caring for diverse patients Posted April 11, 2023 by ,Penn State Health News Prolung Ngin , a certified registered nurseanesthetist (CRNA) at Penn State Health Milton S.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operating room supplies. The required parts are an operating room anesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps. The video is posted here.
A doctor or a nurse? The medical center previously had an anesthesia staff that included both MDs and CRNAs (Certified Registered NurseAnesthetists). A quote from the Medscape article read: “Adam Dachman, MD, a surgeon at the hospital, speaking for himself, said he has no problem using nurseanesthetists.
Anesthesiologists still work in hospital operating rooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. The job of a certified nurseanesthetist was listed as #11 on the Best Paying Jobs list.
Certified Registered NurseAnesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. With this information in mind, CRNAs collaborate with surgeons, nurses, and other healthcare professionals to develop personalized anesthesia plans to meet the specific needs of each patient.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operating rooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
Without a doubt, the operating room (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. Still, with the OR a prime revenue-generator for any hospital, its operation should be scrutinized to see where cost-savings might be implemented. So, why aren’t hospitals developing and expanding the OR?
Dawn Bent, DNP, MSN, CRNA , didn’t choose to be a nurseanesthetist as much as the profession chose her. She was working as an ICU nurse for eight years when one of the anesthesiologists that she worked with told her: “I think you would be a great nurseanesthetist.”
Additionally, the anesthesiologist leads teams of certified registered nurseanesthetists ( CRNA s) and certified anesthesiologist assistants (CAAs). An anesthesiologist is a medical doctor who plays a critical role in the preparation, execution, and recovery stages of surgery.
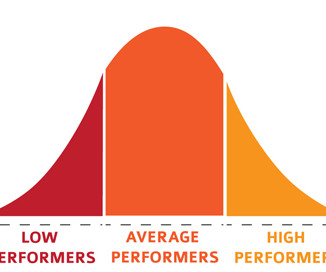
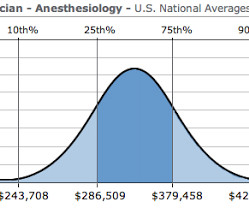
Certified Registered NurseAnesthetists (CRNAs): Equally noteworthy, 51% of CRNAs earn over $226,000 annually, demonstrating the competitive compensation in this segment of the workforce. Specialties of Interest: Understanding which specialties are attracting anesthesia clinicians can inform workforce planning and resource allocation.
In many private practice anesthesia groups, physician anesthesiologists supervise multiple nurseanesthetists in multiple operating rooms. Physician anesthesiologists pay their nurseanesthetists as employees as well as their other expenses, and then divide the profit.
The scrubs are enclosed in a device not dissimilar to a soda machine, and you need your ID to operate it. Empty Operating Room 0655 hours—You don a bouffant hat and a facemask, and enter your operating room. Empty Operating Room 0655 hours—You don a bouffant hat and a facemask, and enter your operating room.
Surgeons work with physician anesthesiologists, with certified nurseanesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists typically spend 90+% of their working hours in the operating room. There are Two Laws of Anesthesia, according to surgeon lore.
million operations from taking place (3). A study on anesthesiology residency programs found that expanding residency programs resulted in significant cost savings for healthcare organizations, considering that the cost per hour of clinical coverage for residents is far lower than that of paying nurseanesthetists overtime (2).
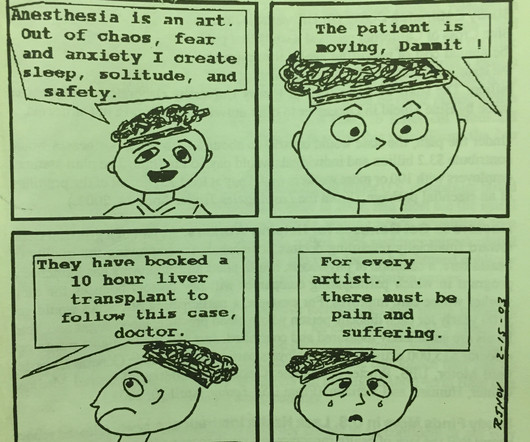
You won’t see us crying, as Dr. Baker is doing in panel 4, but the anesthesiologist’s rapid heart rate and the adrenaline rush in high pressure operating room situations accompany the growth of every anesthesiologist from inexperience trainee to seasoned professional.
You have to get along well with surgeons, the nursing staff, the scrub techs, administrators, and the patients. Their patients are obtunded on arrival to the Post Anesthesia Care Unit (PACU) after surgery, and they rely on the PACU nursing staff to complete the job of anesthesia wake up. Be friendly and personable. Some are not.
Particularly in acute care, the computer keyboard and screen have no place between an anesthesiologist and his patient, an emergency room physician and his patient, an ICU doctor and his patient, or an ICU nurse and her patient. Nurses consistently have their backs to patients as they type, type, type data into computer terminals.
Anesthetist options were limited. Before her surgery, Alexandra reclined awake on the operating room table. You can request more morphine, and the nurse in the recovery room will give it to you.” “Yes. Life is a series of choices. I chose to be my wife’s doctor. It was an opportunity to silence her, and I took it.
More care team anesthesia and more Certified NurseAnesthetists (CRNAs). There will be a paucity of new drugs to change the practice of operating room anesthesia. Hospital systems will have increased incentives to perform anesthetics with cheaper labor.
Each operating room anesthesia location is the epicenter of computerized medical record-keeping machines, computerized Pyxis-style drug storage systems, computerized labeling machines, and bar-code reading billing machines. Acute pain services utilize nerve blocks and other adjuncts to relieve post-operative discomfort.
He is verbal with his mother, but refuses to interact with the anesthesia or nursing personnel. The two hospital guards and the mother donned white operating room coveralls. He refuses to change into a hospital gown, or to remove his long-sleeved sweater. mg/kg midazolam, and.02 02 mg/kg atropine into the patient’s deltoid muscle.
Let’s assume your surgeon is determined to operate urgently, and doesn’t want to wait 6 hours after the patient’s meal. Joining the hospital staff, Nico runs afoul of a grouchy nurseanesthetist calling himself Bobby Dylan, who plays Dylan songs twice a week in a bar called Heaven’s Door.
An operating room anesthesia practice is somewhat akin to being a taxi cab driver. Joining the hospital staff, Nico runs afoul of a grouchy nurseanesthetist calling himself Bobby Dylan, who plays Dylan songs twice a week in a bar called Heaven’s Door. Different payers pay different sums per unit time.
For a long operating room anesthesia case (e.g. Propofol administration requires an experienced clinician, e.g. either an anesthesiologist, a certified registered nurseanesthetist (CRNA), or an emergency medicine physician. Give your patient a dose of Versed before they enter the operating room. Every one of them.
A few non-medical professionals wrote articles in magazines, newspapers, and encyclopedias to explain medical facts, diagnoses, and therapy to the lay public, but the overwhelming majority of the information was only presented to doctors and nurses in the form of medical books and journals.
This likely would lead to an increased role for certified nurseanesthetists (CRNAs), and an eventual increase in the number of schools training CRNAs, but in the short term there would be no way to staff adequate numbers of anesthesia professionals. Risk during an anesthesia career is omnipresent.
General anesthesia is then maintained by the administration of a potent inhaled anesthetic gas such as sevoflurane, supplemented by the intravenous injection of a narcotic such as fentanyl to assure post-operative pain relief. Hibbing also happens to be the hometown of music icon Bob Dylan.
Regarding the appropriate amount of narcotic, I recommend dosing the narcotic as required to treat post-operative pain, and no more. May you, in the words of the Sade song, be a “Smooth Operator.” The number of patients in these series is small, and none of the papers are linked to improved outcomes.
During this COVID crisis, intensive care unit and emergency room doctors and nurses in hotspots like New York City have dangerous, exhausting jobs keeping coronavirus patients alive. A minority of doctors and nurses are saddled with these dangerous around-the-clock jobs battling the disease in ICUs and ERs.
No, it’s not the nurseanesthetists, nor the stress of covering surgeries in the middle of the night, nor the stress of saving patients who are trying to die in front of our eyes during acute care emergencies. In the operating rooms, the patients are brought in by the surgeons. What is this threat?
Will it be a nurse or will it be a physician? Very few patients die in the operating room, but significant numbers die in the weeks that follow. At times, physician anesthesiologists employ certified registered nurseanesthetists (CRNAs) to assist them in what is called the anesthesia care team (ACT) model.
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operating room. Every hospital operating room is equipped with a computer connected to the internet. Other uses of the internet by anesthesiologists in the operating room.
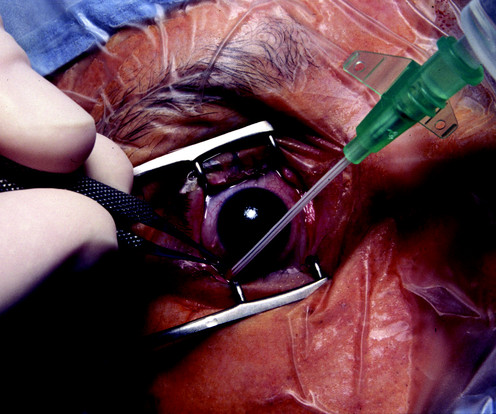
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The patient enters the operating room at 0730 hours. Her last job was as a home health nurse for a registry company.
Anesthesiologists work in operating rooms and intensive care units—acute care settings which demand vigilance, steady hands, and quick thinking. These arenas will be: 1) diagnosis of images, 2) clinics, and 3) operating rooms/intensive care units. What will an AIM robot doctor look like? It’s unlikely it will look like a human.
Are we physicians or are we glorified advanced practice nurses?” In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operating room. Read my column on bullying in the operating room. Are we the ‘captain of the ship’ or is the surgeon?
Louis Imagine this: You’re an anesthesiologist in the operating room at a busy hospital. A team led by an attending anesthesiologist uses remote monitoring to provide evidence-based support to anesthesia colleagues in all the operating rooms. The Barnes Jewish Hospital, Washington University, St.
This technique induced vasoconstriction and resulted in decreased blood loss, and made transfusion and post-operative anemia rare. Our facility, the Plastic Surgery Center in Palo Alto, has two operating rooms. Twin Bair Huggers are used to warm both the lower and upper non-operative fields of the patient’s body.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content