This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In 2021 a nurseanesthetist publication looked at the use of Google Glass by seven nurseanesthetists for display of the vital signs monitor , but there were no quantitative data to examine the significance of the technology. The post SMART GLASSES IN THE OPERATINGROOM appeared first on The anesthesia consultant.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. Evolution of Procedures and Procedural Areas Procedures that used to be hospital-based have increasingly moved into outpatient settings and physician’s offices. Imagine this: It’s the year 2034.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
Today’s post demonstrates making a reusable N95 mask from common inexpensive operatingroom supplies. The required parts are an operatingroom anesthesia mask and a ventilator in-line bacterial/viral filter: The mask assembly is held over your face with elastic straps. The video is posted here.
Without a doubt, the operatingroom (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. So, why aren’t hospitals developing and expanding the OR? link] The Three Anesthesia Staffing Models: The optimal hospital staffing model should: 1. improve efficiencies 2. Permalink
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ The hospital was Watertown Regional Medical Center, located in Watertown, Wisconsin , population 23,861, midway between Milwaukee and Madison. Why did this change happen?
Advanced Practice Provider Spotlight: Certified registered nurseanesthetist shares perspective on caring for diverse patients Posted April 11, 2023 by ,Penn State Health News Prolung Ngin , a certified registered nurseanesthetist (CRNA) at Penn State Health Milton S.
Anesthesiologists still work in hospitaloperatingrooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. The job of a certified nurseanesthetist was listed as #11 on the Best Paying Jobs list.
Certified Registered NurseAnesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. In an operatingroom, the CRNA administers the anesthesia according to the predetermined plan and monitors the patient’s vitals in order to adjust levels as needed.
Dawn Bent, DNP, MSN, CRNA , didn’t choose to be a nurseanesthetist as much as the profession chose her. She was working as an ICU nurse for eight years when one of the anesthesiologists that she worked with told her: “I think you would be a great nurseanesthetist.” Christopher’s Hospital for Children.
To aid you in visualizing yourself in the hospital, I’m substituting the pronoun “you” instead of “I” in the narrative below. You complete your morning bathroom and breakfast routines, and leave your residence at 0630 hours for the hospital. You take the elevator to the third floor and proceed to the locker room.
The Merriam-Webster online dictionary defines private practice as: “a professional business (such as that of a lawyer or doctor) that is not controlled or paid for by the government or a larger company (such as a hospital).” In my community the dentists are all in private practice, as are most of the accountants, psychologists, and attorneys.
Surgeons work with physician anesthesiologists, with certified nurseanesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Anesthesiologists typically spend 90+% of their working hours in the operatingroom. They are: The patient must not move.
We’re entering an era of metrics for physicians, in which the government and hospital systems will collect data to monitor quality and performance. Many hospitals and surgical centers prefer to have an RN place the preoperative IVs. Stick up for the circulating nurse and the scrub tech as well, if necessary.
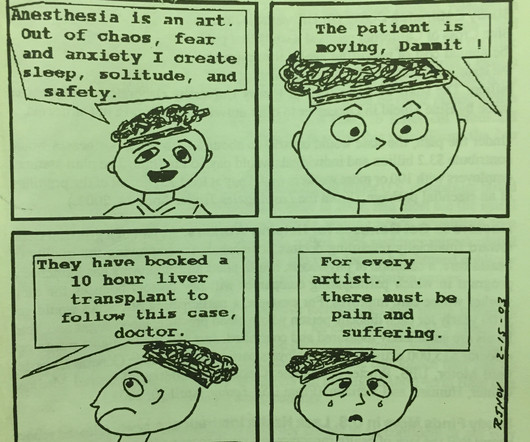
You won’t see us crying, as Dr. Baker is doing in panel 4, but the anesthesiologist’s rapid heart rate and the adrenaline rush in high pressure operatingroom situations accompany the growth of every anesthesiologist from inexperience trainee to seasoned professional.
I agree with him that the current cumbersome EHRs come between doctors and patients during hospital care. My criticisms include: Different EHRs at different hospitals are unable to communicate with each other. If you work at different hospitals with different EHRs, you have to be trained and retrained in multiple EHR platforms.
Dental cases are common, and are frequently referred to a hospital because the typical care systems at an outpatient surgery center or a dental office are inadequate to complete a successful anesthetic. He is verbal with his mother, but refuses to interact with the anesthesia or nursing personnel. mg/kg midazolam, and.02
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. More care team anesthesia and more Certified NurseAnesthetists (CRNAs).
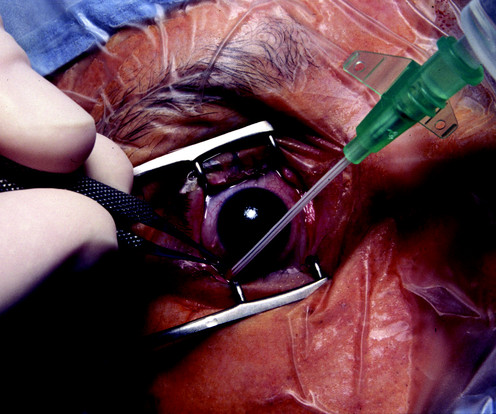
The boy suffers a penetrating open eye injury, and is taken to the nearest hospital. A children’s hospital or a university hospital will have a team of pediatric anesthesiologists with specialized training on call for emergencies. A 3-year-old boy is eating a McDonalds Happy Meal on the lawn of the restaurant. What do you do?
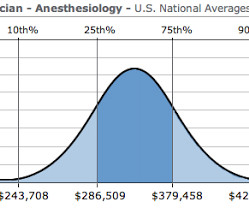
An operatingroom anesthesia practice is somewhat akin to being a taxi cab driver. The Veterans Affairs hospitals are currently pondering a move to allow CRNAs to practice independently without any physician anesthesiologist present. What specific factors determine how high the anesthesiologist’s salary will be?
Each operatingroom anesthesia location is the epicenter of computerized medical record-keeping machines, computerized Pyxis-style drug storage systems, computerized labeling machines, and bar-code reading billing machines. Anesthesia in 2018 is markedly different from anesthesia in the 1990s.
Anesthetist options were limited. Before her surgery, Alexandra reclined awake on the operatingroom table. Her eyes were closed, and she was unaware I’d entered the room. Life is a series of choices. I chose to be my wife’s doctor. It was an opportunity to silence her, and I took it.
This likely would lead to an increased role for certified nurseanesthetists (CRNAs), and an eventual increase in the number of schools training CRNAs, but in the short term there would be no way to staff adequate numbers of anesthesia professionals. Risk during an anesthesia career is omnipresent.
No, it’s not the nurseanesthetists, nor the stress of covering surgeries in the middle of the night, nor the stress of saving patients who are trying to die in front of our eyes during acute care emergencies. This network of patients will serve to keep their clinics and hospitals full and profitable. What is this threat?
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Every hospitaloperatingroom is equipped with a computer connected to the internet. Love it or hate it, the EMR is here to stay.
The Barnes Jewish Hospital, Washington University, St. Louis Imagine this: You’re an anesthesiologist in the operatingroom at a busy hospital. Anesthesiologists at Barnes Jewish Hospital at Washington University in St. What do you do? How do you feel about all this?
Surgeons, anesthesiologists, certified nurseanesthetists, and operatingroomnurses are barely working at all now, for the fourth consecutive week. Elective surgery has been cancelled at the hospital I work at, Stanford University Hospital, per the CMS edict.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The patient enters the operatingroom at 0730 hours. The patient consents. Can this scenario occur?
A typical hospital will have dozens of other anesthesia providers working in the same building. In an anesthesia care team, a physician anesthesiologist supervises up to four operatingrooms and each operatingroom is staffed with a certified registered nurseanesthetist (CRNA). Sound scary?
THE JULY EFFECT AND THE NOVEMBER EFFECT: In American teaching hospitals, newly minted doctors begin internships each July. The term “July Effect” was coined to describe this shift change in academic hospitals each July, when the arrival of inexperienced doctors may increase the risks of medical care.
Anesthesiologists work in operatingrooms and intensive care units—acute care settings which demand vigilance, steady hands, and quick thinking. These arenas will be: 1) diagnosis of images, 2) clinics, and 3) operatingrooms/intensive care units. What will an AIM robot doctor look like?
You’re on your at the hospital, sometimes on weekend nights, and sometimes at 3 a.m. If there’s a hospital location or an anesthesia group you’re particularly interested in, but they are not advertising a job opening. Find out who the leader of the group is, and call the operatingroom or the anesthesia company’s phone number.
Norman Shumway MD PhD, a Stanford surgical professor and legend, invented the heart transplantation procedure and performed the first heart transplant in the USA on January 6, 1968 in operatingroom 13 of Stanford University Hospital. Upon arrival at the airport in the donor city, an ambulance transported us to the hospital.
More likely to work part-time, and with a nurseanesthetist care-team delivery system. The authors of this paper proposed regulations to include: no further on-call duties for those aged 60 and older, no further high-acuity cases for those aged 65 and older, and retirement from operatingroom clinical practice at age 70.
Here are some general steps that might be considered: Alert the medical team: The anesthesiologist or healthcare providers in the operatingroom need to be notified immediately about the patient’s deteriorating condition. The surgeon and additional medical personnel may also be called upon for assistance. No, not really.
No data exists to support that initial video laryngoscopy is safer or more effective than direct laryngoscopy when used by anesthesiologists in operatingrooms. Joining the hospital staff, Nico runs afoul of a grouchy nurseanesthetist calling himself Bobby Dylan, who plays Dylan songs twice a week in a bar called Heaven’s Door.
Our facility, the Plastic Surgery Center in Palo Alto, has two operatingrooms. At times the second room is not occupied, and a solo anesthesiologist is the only anesthesia professional present on site and must be prepared to handle any and all emergencies. Hibbing also happens to be the hometown of music icon Bob Dylan.
A total of 266 cases of brain damage or death during anesthesia care in the operatingroom under the care of a solo anesthesiologist occurred. All the anesthesiologists were single practitioners, that is, they were not part of an anesthesia care team with a nurseanesthetist. Resist these pressures.
3) Physicians from a Thai teaching hospital reviewed 44,339 emergency surgery patients from 2003 to 2011, and found the incidence of perioperative cardiac arrest in emergency surgery was 163 per 10,000 cases. A 9-year survey in a Brazilian tertiary teaching hospital. Anesthesiologists will continue to be challenged. References: 1.
Maggie is paralyzed from the neck down— a ventilator-dependent quadriplegic—and is hospitalized in a private room. In 8 scenes of in-hospital cardiac arrest, 7 of the 8, or 88% of the patients survived, compared to survival rates of 23.9% But how about singing the sexual song in the operatingroom? Remarkable!
In contrast, other operatingroom professionals are usually relaxed and winding down at this time, because the surgical procedure is finished. She walked out of the hospital two days later. If an anesthesia care team is attending to you, how many rooms is each physician anesthesiologist supervising?
Such cases sometimes present to a pediatric hospital for anesthetic care, but at times the child will be treated in a dental office. At this point, the anesthesiologist can take the patient away from the parent and proceed into the operatingroom, where either an intravenous anesthetic or an inhaled sevoflurane anesthetic can be initiated.
CASE TWO: A 55-year old female is scheduled for a facelift at a freestanding plastic surgery center operatingroom. She is transferred to a local hospital and admitted to the intensive care unit. Abdominal surgery and general anesthesia in this patient population are not without risk, even with optimal anesthetic care.
He walked out the hospital alive and well. When a bad outcome like this occurs in a hospital or surgery center, a facility’s Quality Assurance Committee examines the details of the case—not to assign blame—but to identify flaws in patient care systems which must be improved in the future.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content