This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Modern tools designed for anesthesia documentation and billing accuracy can reduce missed charges and improve coding precision. A mix of retiring specialists, increasing demand for surgical procedures, and a limited residency pipeline is driving this shortage. Hospitals must find ways to maximize efficiency with fewer team members.
The operating room team today consists of multiple professionals working in collaboration, including the surgeon, the scrub tech, the circulating nurse, and the anesthesia MD or CRNA. Who is the Captain of the Ship in the operating room, the surgeon or the anesthesiologist? The intern failed to irrigate the eye.
Securing admission into a Certified Registered Nurse Anesthetist (CRNA) program is no small feat. With a rapidly growing demand for CRNA professionals and a surge in applicants, the competition has become fiercer than ever before. Ideally, you should begin preparing by researching CRNA programs extensively.
Every year in January, we celebrate CRNA week. Last week, I encounter a patient that I’ve taken care of twice before (how likely is it amongst 30 CRNAs at the hospital that I get to take care of him 3 times in a row?). Another patient required extra TLC, explanations and a calming presence prior to the induction of anesthesia.
There are four classes of APRNs: certified nurse midwife (CNM), clinical nurse specialist (CNS), certified nurse practitioner (CNP), and certified registered nurse anesthetist (CRNA). Though all APRNs undergo extensive training to achieve their advanced degree, each type obtains a different skillset, with CRNAs focused on anesthesia care.
Certified Registered Nurse Anesthetists (CRNAs) serve an irreplaceable function on medical teams across the country. They play a crucial role in healthcare by ensuring patient safety and comfort before, during, and after surgical procedures. To begin, it’s essential to understand the role of a CRNA.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population). of the population).
CRNA Students Marie Richardson, Nina Marino and ,, Mamawa Hollendyke , MSN, RN received a visit from Pa. s Nurse Anesthesia program, sharing their nursing backgrounds and why they were particularly interested in York's program. After discussing the CRNA profession and touring the simulation lab, Sen.
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operating rooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
In July 2020 the Food and Drug Administration (FDA) approved the intravenous benzodiazepine remimazolam (Byfavo, Acacia Pharma) for use in sedation for procedures of 30 minutes or less. remimazolam propofol For use in procedural sedation, remimazolam will not replace Versed, but rather will aim to replace propofol.
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). The first surgery today is a procedure devised to treat obstructive sleep apnea, a procedure called a maxillary-mandibular osteotomy. You take the elevator to the third floor and proceed to the locker room.
Let’s look at a case study which highlights a specific risk of general anesthesia at a freestanding surgery center or a surgeon’s office operating room, when the anesthesiologist departs soon after the case is finished. The assessment is ASA II, and the plan is general endotracheal anesthesia. The surgery concludes at 1630 hours.
Anesthesia is a hands-on specialty. Anesthesia is said to be “99% boredom and 15 panic,” because 99% of the time patients are stable, yet 1% of the time, especially at the beginning and the end of anesthetics, urgent or emergency circumstances could threaten the life of the patient. Love it or hate it, the EMR is here to stay.
I entered three anesthesia consultations into CHATGPT, one preoperative, one intraoperative, and one postoperative. Medications may need to be adjusted or temporarily stopped to minimize potential risks during the procedure. This could indicate a cardiac event or a complication related to the anesthesia.
He writes, “Our specialty, anesthesia, has suffered an identity crisis for decades. One day I was scrubbed in as a retractor-holding medical student on a 12-hour esophagectomy, and at the conclusion of the procedure the attending surgeon removed his gloves and gown and left the room to talk to the family. Why would I say this?
A 2013 study in Anesthesiology states, “Despite the fact that a surgical procedure may have been performed for the appropriate indication and in a technically perfect manner, patients are threatened by perioperative organ injury. Will it be a nurse or will it be a physician? This is an important question. Why do patients die?
The study looked at malpractice closed claims and found: 1) Outcomes remained poor in malpractice closed claims related to difficult tracheal intubation; 2) The incidence of brain damage or death at induction of anesthesia was 5.5 A surgical airway is an invasive airway via the front of the patient’s neck into their trachea.
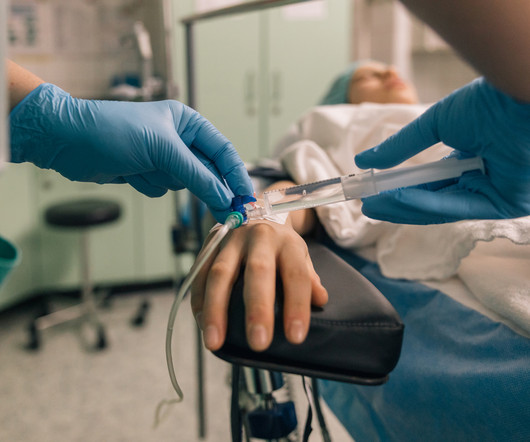
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. The ET tube is a conduit to safely transfer oxygen and anesthesia gases into and out of the lungs. Extubation is risky business.
If something dire goes wrong during anesthesia and surgery and the flow of oxygen to the brain is cut off, an anesthesia practitioner has about five minutes to diagnose the cause of the problem and treat it. The good news is that catastrophic events causing sudden drops in oxygen levels are very rare during anesthesia.
Last November, two hospitals in Portland, Oregon, reportedly had to cancel several hundred procedures—nearly all nonemergency surgeries—due to a shortage of anesthesia providers.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content