This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Who is the Captain of the Ship in the operatingroom, the surgeon or the anesthesiologist? The Captain of the Ship doctrine was a 20 th century legal doctrine which held that, in an operatingroom, the surgeon was “liable for all actions conducted in the course of the operation.”
This was a landmark paper on the topic of anesthesiologist:CRNA staffing ratios, which documented that having physician anesthesiologists direct three or four operatingrooms simultaneously for major noncardiac inpatient surgical procedures increased the 30-day risks of patient morbidity and mortality.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. Imagine this: It’s the year 2034.
When you enter a hospital or surgery center for a surgery and an anesthesia professional approaches you prior to your surgery, that professional could be a physician anesthesiologist, a Certified Registered Nurse Anesthetist, or an Anesthesia Assistant (AA). Meanwhile, the CRNAs are the ones that are administering the anesthesia.
Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10. Then we’ll roll down the hallway into the operatingroom. You may have nausea after generalanesthesia.
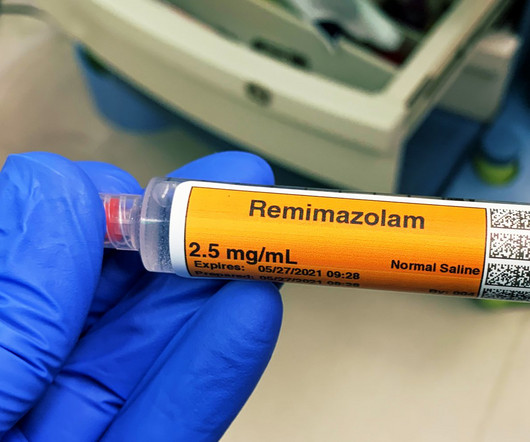
For a long operatingroomanesthesia case (e.g. Propofol administration requires an experienced clinician, e.g. either an anesthesiologist, a certified registered nurse anesthetist (CRNA), or an emergency medicine physician. Give your patient a dose of Versed before they enter the operatingroom.
Anesthesiologists still work in hospital operatingrooms, but their expertise is also needed in other places, including invasive radiology, gastrointestinal endoscopy, electrophysiology and more. The most popular posts for laypeople on The Anesthesia Consultant include: How Long Will It Take To Wake Up From GeneralAnesthesia?
An operatingroomanesthesia practice is somewhat akin to being a taxi cab driver. Just as taxi cab drivers are being supplanted by Uber and Lyft, cheaper models of anesthesia care are popping up, and the penetration of these models into the future marketplace is unknown. Will I Have a Breathing Tube During Anesthesia?
Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Major adverse events seldom occur during the middle of a general anesthetic of long duration on a healthy patient. Love it or hate it, the EMR is here to stay.
Let’s look at a case study which highlights a specific risk of generalanesthesia at a freestanding surgery center or a surgeon’s office operatingroom, when the anesthesiologist departs soon after the case is finished. The patient enters the operatingroom at 0730 hours. The patient consents.
The most invasive type of airway tube used in anesthesia is called an endotracheal tube, or ET tube. At the onset of generalanesthesia anesthesiologists place an ET tube through the mouth, past the larynx (voice box), and into the trachea (windpipe). Why Did Take Me So Long To Wake From GeneralAnesthesia?
In an anesthesia care team, a physician anesthesiologist supervises up to four operatingrooms and each operatingroom is staffed with a certified registered nurse anesthetist (CRNA). In many hospital operatingrooms, a solitary physician anesthesiologist attends to his or her patient alone.
In the late 1970’s I was a third-year medical student at a prominent Midwestern medical school, where an unspoken rank system existed in the operatingroom. Read my column on bullying in the operatingroom. It’s true that surgeons bring the patients to the operatingroom for surgery. Hold your heads high.
INTRAOPERATIVE DECISION A 60-year-old man with a history of hypertension is having a knee arthroscopy surgery under generalanesthesia. The surgical team will be assembled, and the child will be transferred to the operatingroom for further assessment and management. Will I Have a Breathing Tube During Anesthesia?
This is what the anesthesia experience is like for most patients: You show up for surgery, and some anesthesia professional you’ve never met or talked to appears 10 minutes before you are to be wheeled into the operatingroom. The anesthesia professional might be an MD, a CRNA, or both a MD and a CRNA might be involved.
Very few patients die in the operatingroom, but significant numbers die in the weeks that follow. In this model, an MD anesthesiologist supervises up to four CRNAs who work in up to four different operatingrooms simultaneously. Are CRNAs and anesthesiologists equals? Mortality” means a patient death.
Have the Stanford Emergency Manual 5 in your operatingroom suite, and ask a registered nurse to recite the Cognitive Aid Checklist for HYPOXEMIA to you, to make sure you haven’t missed something. If an anesthesia care team is attending to you, how many rooms is each physician anesthesiologist supervising?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content