This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The CSFA is not just a passive participant in the operating room; they are an active collaborator who anticipates the surgeons needs, manages surgical instruments, and assists with critical tasks such as suturing, tissue manipulation, and hemostasis (control of bleeding). Handling and passing surgical instruments to the surgeon.
Surgical care remains one of the most significant drivers of overall hospital cost—yet the medical readiness of complex surgical patients is often overlooked in financial and operational planning. Moreover, these unrecognized or underrecognized secondary diagnoses reduce operating room efficiency by leading to cause delays and cancellations.
From sterile processing and perfusion services to intraoperative neuromonitoring (IONM) and surgical assistants, hospital surgical support teams are the unsung heroes behind every successful operation. Lowers the likelihood of post-operative complications related to neurological function. What Is Hospital Surgical Support?
Today, anesthesiologists and healthcare leaders face mounting challenges that threaten both the profession and patient care. Here are five alarming numbers—and how smarter operational and clinical tools can help. Here are five alarming numbers—and how smarter operational and clinical tools can help.
Who is the Captain of the Ship in the operating room, the surgeon or the anesthesiologist? The Captain of the Ship doctrine was a 20 th century legal doctrine which held that, in an operating room, the surgeon was “liable for all actions conducted in the course of the operation.”
There is a national shortage of anesthesiologists with more demand than supply. Complicating this picture is the level of unhappiness among anesthesiologists and CRNAs. Anesthesia has a prominent role in OR Governance and perioperative operations. Anesthesia providers in most organizations feel undervalued and unappreciated.
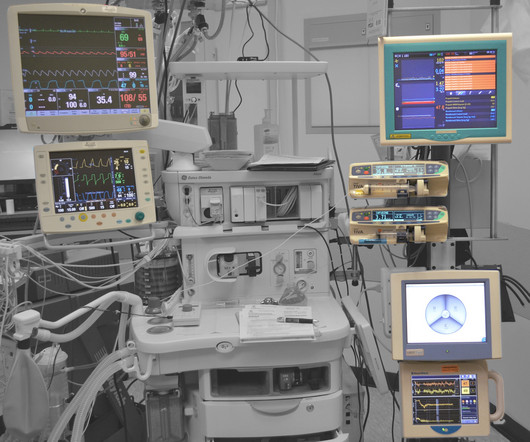
Anesthesiologists watch vital sign monitors continuously in the operating room every day, and have more experience following vital sign abnormalities minute-to-minute than other physicians. The blood oxygen level, or oxygen saturation level, is equivalent to what a pulse oximeter measures in the operating room. Kennedy Jr.
JAMA Surgery published the study “ Association of Anesthesiologist Staffing Ratio With Surgical Patient Morbidity and Mortality ” on July 22, 2022. The physician-CRNA team, otherwise known as an anesthesia care team, is a model strongly supported by the American Society of Anesthesiologists.
A looming shortage of anesthesiologists globally may affect the accessibility of healthcare in the next ten years. The American Association of Medical Colleges predicts that there will be a workforce gap of as many as 12,500 anesthesiologists in the United States by 2033 (3). million operations from taking place (3).
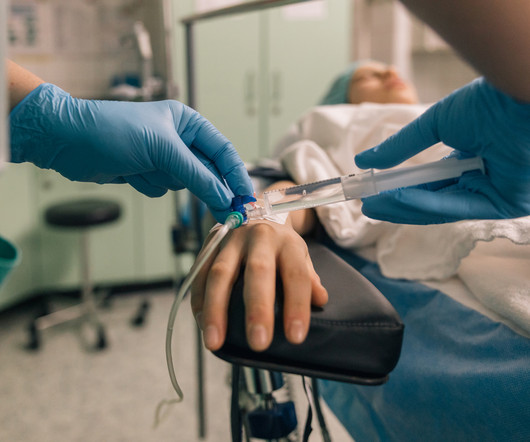
Salem Anesthesia is fortunate to have the best Anesthesiologists on our team. A vital member of this team is the anesthesiologist. A vital member of this team is the anesthesiologist. An anesthesiologist is a medical doctor who plays a critical role in the preparation, execution, and recovery stages of surgery.
On March 28, 2021 the anesthesia world in the United States was rocked by the headline: “ Wisconsin Hospital Replaces All Anesthesiologists With CRNAs. “ Is this a watershed moment for the profession of physician anesthesiologists? Are CRNAs going to replace MD anesthesiologists all over America, changing the profession forever?
What qualities define an outstanding anesthesiologist? Some were academic professors, some were trainees at a university, and some were community anesthesiologists either in my group or in other anesthesia companies. Rather, I’m choosing to list the qualities I’ve witnessed that make physician anesthesiologists stand out as leaders.
One of my readers asked me to describe a day in the life of an anesthesiologist, as he was considering a career in anesthesiology. The scrubs are enclosed in a device not dissimilar to a soda machine, and you need your ID to operate it. Because anesthesiologists do not scrub in a sterile fashion, it’s OK to wear your watch and ring.,
We also had the President of the New York State Society of Anesthesiologists, Dr. Jason Lok, and Dr. John Fiadjoe, Executive Vice Chair of Anesthesia at Boston Children’s Hospital and Director of the American Board of Anesthesiology, joining us at the conference. Attendees for the annual meeting even stayed until the end on Sunday!
Anesthesia emergencies are anxiety-producing for both experienced and inexperienced anesthesiologists, but experienced doctors are more likely to know exactly what to do and what not to do. Perioperative” means “the time around an operation”—specifically the preoperative, postoperative, and intraoperative times.
Anesthesiology residents play an important role in the operating room (OR), assisting with patient care while also undergoing rigorous training to become skilled anesthesiologists. As residents continue to learn and grow under their supervisor, they are entrusted with an increasing number of responsibilities in the operating room.
This will require an operating room staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. The Center for Anesthesia Workforce Studies estimates that current clinically active anesthesia professionals are made up of 43,500 anesthesiologists, 50,000 nurse anesthetists, and 3,200 anesthesiologist assistants.
Mayim Bialik may be the straw that broke the camel’s back once and for all for Anesthesiologists throughout the world. On Friday night’s Jeopardy during the meet and greet portion, Bialik referred to one of the contestants who is an anesthesiologist as “just an anesthesiologist”, and not a surgeon.
In the control group of this study, each anesthesiologist would use a traditional ultrasound screen to visualize the artery. The anesthesiologist must look up to see the ultrasound machine, while he is working on the patient’s wrist. Smart glasses are being studied in aviation. Let’s look at this last point.
Will Gawande change the future for anesthesiologists? Let’s look at these three proposed Gawande changes, and how they affect the future for anesthesiologists: Taking out the trash. From the exam room to the operating room, doctors today follow a clear set of protocols that Dr. Gawande helped establish. Creating a checklist.
What’s the difference between a physician anesthesiologist and a nurse anesthetist? There is no fork in the career path that makes a busy Certified Registered Nurse Anesthetist (CRNA) automatically inferior to a medical doctor anesthesiologist in hands-on skills. The answer: internal medicine.
News and World Report credited anesthesiologist with another honor: the highest paying job in their 2018 Best Paying Jobs survey. Regarding the #1 job, physician anesthesiologist , the article states, “the breadth of the profession has dramatically expanded in the last decade.
[link] Efficient Case Scheduling - Secret to a Well-Run OR Operating room costs can be categorized as fixed or variable. Variable costs are largely driven by caseload and associated labor costs that occur outside of normal operational hours. Anesthesiologists, surgeons, and other clinical team members must arrive on time.
At one New York medical center, intense clinical demands and provider fatigue have inspired one anesthesiologist to push the boundaries of clinical medicine. Dr. Mac “McGrath” Millerstein, a cardiothoracic anesthesiologist, has intubated countless patients with COVID over the last several weeks.
You utilize the current multimodal strategies for operating room anesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% Neurosurgeons have taken him to the operating room to drain the hematoma and decompress the spinal column. How can an anesthesiologist make such an error?
In recent years, engineers have developed closed-loop AI machines that can administer appropriate doses of anesthetics without human input , as described in The Washington Post article, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Thus, we might ask, ‘What happens to the operator/clinician involved?’
The Realizing Improved Patient Care through Human-Centered Design in the Operating Room (RIPCHD.OR) learning lab uses a socio-technical approach incorporating human factors engineering and evidence-based design principles to create an optimal ergonomically sound operating room that results in improved patient and staff safety.
For patients with restless leg syndrome undergoing anesthesia, the involuntary leg movements and discomfort can pose challenges for anesthesiologists, requiring specialized techniques and considerations to ensure safe and effective anesthesia administration.
Additionally, academic anesthesiology is unique because we often schedule a pre-operative phone call [usually the day before surgery when we get our assignments] with the residents in order to discuss the anesthetic plan and direct educational topics for the day [see below].
Surgeons work with physician anesthesiologists, with certified nurse anesthetists (CRNAs), or with an anesthesia care team that includes both physician anesthesiologists and CRNAs. Most surgeons’ comprehension of what anesthesiologists are doing is limited. Anesthesiologists win the tally for most operating room hours per week.
Miller 2 Direct Laryngoscope Video Laryngoscope When it’s time to insert an endotracheal tube, for decades anesthesiologists have utilized a direct laryngoscope. Direct laryngoscopy (DL) is a difficult skill to acquire, but all anesthesiologists become masters of it. Enter the video camera, which changed surgical practice.
Without a doubt, the operating room (OR) brings in the lion’s share of a hospital’s revenue, amounting to as much as 70% or more. Still, with the OR a prime revenue-generator for any hospital, its operation should be scrutinized to see where cost-savings might be implemented. So, why aren’t hospitals developing and expanding the OR?
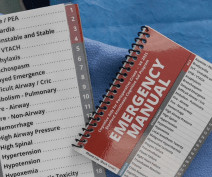
CardioPulmonary Resuscitation in the Operating Room The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operating room. A printable version of the Stanford Emergency Manual is available online for free.
Are anesthesiologists on the verge of being replaced by a new robot? THE iCONTROL-RP ANESTHESIA ROBOT On May 15, 2015, the Washington Post published a story titled, “We Are Convinced the Machine Can Do Better Than Human Anesthesiologists.” Why is this robotic device only a small step toward replacing anesthesiologists?
Why should anesthesiologists be any different? In many private practice anesthesia groups, physician anesthesiologists supervise multiple nurse anesthetists in multiple operating rooms. Physician anesthesiologists pay their nurse anesthetists as employees as well as their other expenses, and then divide the profit.
Save these documents and present them to future anesthesiologists. Inform future anesthesiologists regarding your history of prolonged sedation, and they can make adjustments in their drug delivery and techniques to attempt to avoid the same problems. Don’t be afraid to inform your anesthesiologist.
Primary Consultant Anesthesiologist The “Preoperative Evaluation” chapter in our Bible, Miller’s Anesthesia , is 80 pages long—one of the longest chapters in the book. As a double-boarded anesthesiologist and internal medicine doctor, preoperative evaluation has been my area of interest and expertise for decades.
The inside of the healthcare facility will be cleaned prior to any patient care, and will be recleaned after each patient leaves an operating room. Our county and state health administrations have noted a decline in the incidence of COVID cases, and have authorized a reopening of elective surgery.
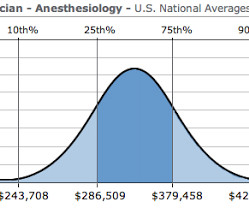
How much money does an anesthesiologist earn? What is a physician anesthesiologist’s salary in today’s marketplace? I recently received an email from a medical student who was considering anesthesia as a career specialty, but his concern was: is the bottom about to fall out for anesthesiologists’ salaries?
Peter, MN – Physician on FIRE , an anesthesiologist and financial blogger , recently hit the magical goal of Financial Independence and Retire Early (FIRE) in his mid 40s. Once he achieved ‘FIRE status’ JACHO and hospital administration determined he was too much of a fire risk to be in the operating room.
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operating room (OR) to the post-anesthesia care unit (PACU). An anesthesiologist can easily make a diagnosis of inadequate breathing if a patient is connected to a pulse oximeter.
My friend, colleague, and President of the company I work for, the Associated Anesthesiologists Medical Group in Palo Alto, California, wrote an excellent column describing Locker Slammers for the American Society of Anesthesiologists Monitor (September 1, 2018; Volume 82, Number 9). Read on–you won’t be disappointed.
As the anesthesiologist, it’s your job to make the correct diagnosis and act promptly to save your patient. You’re a Medical Director or medical educator, and you’re scheduled to deliver a lecture on the management of two or three common operating room emergencies. An anesthesia emergency occurs without warning.
I’m writing this from the perspective of a busy clinician who has worked as an anesthesiologist in California in both private practice and at a major university hospital for over 30 years. There will be a paucity of new drugs to change the practice of operating room anesthesia. An on-call anesthesiologist came to work at 7 a.m.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content