This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The operatingroom is a fast-paced, high-stakes environment where precision, teamwork, and vigilance are non-negotiable. Safe surgical care demands seamless collaboration between surgeons, nurses, techs, and anesthesia providers, so that we can achieve excellent outcomes. 4 But what about operatingroom nurses specifically?
OperatingRoom (OR) nurses, also known as perioperative nurses, play an essential role in surgeries. They are responsible for maintaining a sterile environment, assisting surgeons, and ensuring patient safety throughout the surgical process. What Does an OR Nurse Do?
Any step which enhances safety can be seen as a valuable change. AEROGLASS in aviation A recent review states , “The AEROGLASS turnkey smart glass solution provides general aviation pilots a true 3D, 360° view of navigation and safety features. Smart glasses are being studied in aviation.
Many factors affect the operatingroom (OR) and surgery success, ranging from patient-related factors to resource-related factors to even clinician-related factors. In the operatingroom (OR), teamwork is crucial for ensuring patient safety. The American Journal of Surgery, vol. 24–30, [link] 2.
Anesthesiology residents play an important role in the operatingroom (OR), assisting with patient care while also undergoing rigorous training to become skilled anesthesiologists. Their responsibilities encompass a range of tasks, from preoperative evaluations to the administration of anesthesia and postoperative care.
Challenge 1: Avoiding Governance Issues With Proven Strategies If ORs and the departments that support them are not aligned or communicating, patient throughput, patient safety, and the facility’s financial sustainability are all threatened. In the surgery center specifically, Sullivan’s team helped establish an operatingroom committee.
This will require an operatingroom staffed with a surgeon, a nurse, a scrub technician, and an anesthesia professional. If the current trend of inadequate numbers of anesthesia clinicians in the United States is not reversed, this insufficient supply will be a major problem. of the population).
Annual meeting Vice-Chair Dr. Engy Said put together a fantastic point-of-care ultrasound and regional anesthesia workshop on Thursday. Mason as well as some other inspirational anesthesiologists, see these video interviews posted by Dr. Allison Fernandez for the Women of Impact in Anesthesiology project.
Post-Anesthesia Care Unit (PACU) nurses are the unsung heroes of surgery centers. Their critical role begins as soon as patients leave the operatingroom and continues until they are stable enough to recover at home or in a hospital room. Their role in maintaining the flow of operations cannot be overstated.
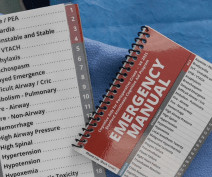
An anesthesia emergency occurs without warning. You need the ultimate anesthesia emergency guidebook. That ultimate guidebook is the S tanford Emergency Manual of Cognitive Aids for Perioperative Critical Events S , written by the Stanford Anesthesia Cognitive Aid Group. Your patient’s vital signs are dropping.
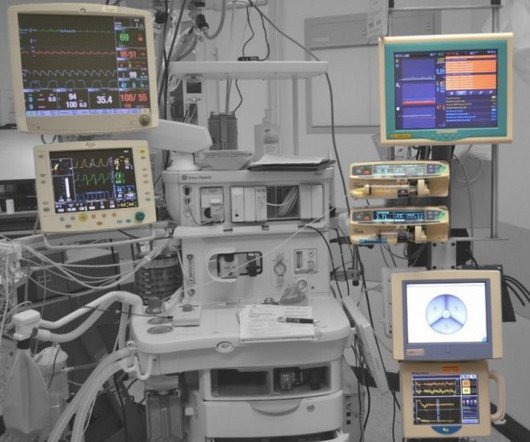
Anesthesia is not the career for you if you like to sleep late—surgery always begins at 0730 hours). Empty OperatingRoom 0655 hours—You don a bouffant hat and a facemask, and enter your operatingroom. Your hospital contains multiple operatingrooms, and today you are in room #10.
CardioPulmonary Resuscitation in the OperatingRoom The Stanford Emergency Manual has become an essential reference for anesthesiologists. One can also order a laminated 8½ x 11½-inch version of the Manual to hang in each operatingroom. Both were published in the journal Anesthesia and Analgesia.
The February 2020 edition of Anesthesiology , our specialty’s preeminent journal, published an article on robotic anesthesia. 1 The accompanying editorial by Dr. Thomas Hemmerling was titled “Robots Will Perform Anesthesia in the Near Future. ” robotic) anesthesia is at least as good as the best human anesthesia.
They play a crucial role in healthcare by ensuring patient safety and comfort before, during, and after surgical procedures. Anesthesia is a vital tool in modern medicine and CRNAs serve as experts in providing this medical service to patients. To begin, it’s essential to understand the role of a CRNA.
The joint statement also said that “facilities should use available testing to protect staff and patient safety whenever possible and should implement a policy addressing requirements and frequency for patient and staff testing.” Everyone in the healthcare facility will be wearing masks.
Anesthesia departments are crucial to the success of operatingrooms (ORs). Ensuring your anesthesia team excels in both areas is vital. Here are five warning signs that your anesthesia team might be underperforming: 1. Here are five warning signs that your anesthesia team might be underperforming: 1.
In the highly specialized field of plastic surgery, having a reliable and skilled team is essential to delivering top-notch results and ensuring patient safety. Their responsibilities include: Preoperative Preparation: Ensuring the operatingroom is ready, sterilizing instruments, and preparing patients for surgery.
Some of their main tasks include: Preparing the OperatingRoom : Surgical assistants ensure all equipment is sterile and ready. Surgical assistants streamline the entire process from pre-op to post-op. This reduces patient time under anesthesia and the risk of complications. We serve Maryland, Washington D.C.,
Imagine this scenario: You’ve just finished anesthetizing a patient in a hospital setting, and the patient now requires transport from the operatingroom (OR) to the post-anesthesia care unit (PACU). This is a reasonable policy, but what if anesthesia patient transport to the PACU lasts 4 minutes and 59 seconds (i.e.
You utilize the current multimodal strategies for operatingroomanesthesia and postoperative pain reduction, including an ultrasound-guided adductor canal block with 0.5% The patient does well, and is discharged from the PostAnesthesia Care Unit in excellent condition. He’s right. What happened?
More care team anesthesia and more Certified Nurse Anesthetists (CRNAs). Rather than physician anesthesiologists personally performing anesthesia, expect to see CRNAs supervised by physician anesthesiologists in an anesthesia care team, or in some states, CRNAs working alone. Anesthesia personnel will be in great demand.
When a patient decompensates emergently at a freestanding ambulatory surgery center or in an operatingroom at a doctor’s office, the facility will call for an ambulance staffed with EMT personnel. Pulmonary edema fluid filled her lungs and filled the hoses of the anesthesia machine.
His address, “We Need Leaders,” tackled the issues of improvements in patient safety and the multiple levels of leadership that made those advances possible. We don’t need leaders just for the advancement of patient safety; right now our specialty desperately needs leaders on every front. They deliver clinical anesthesia, period.
Having properly certified assistants at surgery usually makes the operation go faster, safer and smoothly. Having expert assistance can translate into shortening the time needed for anesthesia, increasing the safety of the procedure, reducing the surgical complication rates, and thus decreasing operatingroom costs.
Because the spaceship is more than 200 days away from Earth, the physicians instruct the crew to proceed with surgery and anesthesia in outer space. How will astronauts conduct general anesthesia and surgery in outer space? Protocols regarding how to accomplish anesthesia in outer space exist in the medical literature.
However, the operating tables market is growing and will reach US $1,043.41 With this forecasted growth rate, you need to know how to quickly find the best surgical tables for your operatingroom (OR). But first, let us define an operating table and explore some characteristics. What is an operating table?
The challenges for operatingroom (OR) managers are universal: improving surgical workflow efficiency while providing high-quality, reliable, safe patient care. She shares First Case On-Time Starts daily with the staff and to improve visibility of those data points, she posts them on the daily management boards.
With rising anesthesia costs and stagnating reimbursements, ASCs’ margins are thinner than they were even five years ago. What’s the State of the Facility’s Anesthesia Provider Relationship? Understanding the relationship between the ASC and its anesthesia provider is essential, particularly if a stipend is involved.
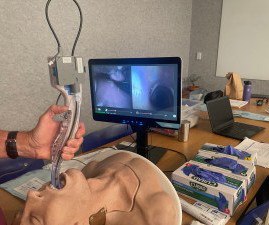
The intraoperative period (green in Fig 1) is of particular interest, not least because these are the processes that utilize the operatingroom (OR) and a large part of a hospital’s expenditure. They look to see if everything is ready for anesthesia, including the video-guided system this anesthesiologist likes to use.
Patient safety should be at the top of everyone’s priority list, and when everything is viewed through that lens, then we realize that every department assisting surgical services adds value and should be given the proper consideration for how they affect our patient outcomes. And we can’t operate without sterile instruments.
Just before the start of anesthesia, a patient may hear the operatingroom nurse saying, “Think of a nice dream as you go off to sleep.” While these statements are intended to soothe patients during a stressful time, they gloss over this critical fact: Anesthesia is not like normal sleep at all.
I’m writing this review to inform anesthesia providers and laypersons regarding developments in the field of anesthesiology. Vladimir Nekhendzy, Clinical Professor of Anesthesiology and Otolaryngology, Stanford University School of Medicine, and Past President of the Society for Head and Neck Anesthesia, is the inventor of the Spiro device.
Anesthesia is a hands-on specialty. Anesthesiologists could chat with the surgeons and/or nurses, make an occasional phone call, and at times read materials they brought with them into the operatingroom. Since the development of the internet, anesthesia practice has changed forever.
Every anesthesia provider must learn to free-solo anesthesia early in his or her career. The 2018 movie Free Solo showcases Alex Honnold as he became the first person to free solo climb the 3000-feet high El Capitan wall of granite in Yosemite National Park without ropes or safety gear. Working alone may be less safe.
Anesthesiology is a wonderful profession, as I have described in many previous posts on theanesthesiaconsultant.com. But nothing is perfect, and anesthesia has one threat which could in time undermine the entire specialty. In the operatingrooms, the patients are brought in by the surgeons. What is this threat?
In particular, there are unique considerations for patients undergoing cancer treatment, especially radiation therapy, who need anesthesia. A fraction of patients may need to undergo intraoperative radiation therapy, which carries a whole additional set of unique anesthesia and other clinical considerations.
You’ve graduated from a residency program in which you learned the nuances of preoperative, intraoperative, and postoperative anesthesia practice. You believe the patient is high risk in terms of his airway, his breathing, his cardiac status, and his potential for post-operative complications. You’re in charge of the anesthetic.
Data exists that intravenous caffeine may be effective in assisting the awakening of patients following general anesthesia. The safety of caffeine has been well established, and the energy drink market is expected to reach 83.4 Intravenous caffeine post-surgery is not a new idea. 12-ounce cola contains from 30 to 50 mg.
Post-infrarenal clamping has an incidence of AKI of 5% versus 13% for post-suprarenal clamping. For example, anesthesia may decrease RBF by dropping CO or MAP. Sympathetic stimulation occurs secondary to surgical stress, general anesthesia, hypoxia, hypotension, pain, severe bleeding, and strenuous exercise.
The report recommended that instead of blaming individuals, to instead prevent future errors by designing safety into the system. Some reports reveal only minor issues such as prolonged post-operative nausea and vomiting, or a prolonged PostAnesthesia Care Unit stay. The patient had an immediate cardiac arrest.
Many of you have never heard of Dr. New, and don’t know what he was famous for, but in my opinion he was the Most Valuable Player of the anesthesia ranks in the last one hundred years. Nellcor’s successful production, marketing, and sales efforts of their pulse oximeter changed not just anesthesia practice, but medical practice, forever.
Sugammadex is not cheap (a cost of $100 per 200 mg vial), but since the availability of sugammadex, no anesthesia practitioner should ever have an awake and still-paralyzed patient at the conclusion of an anesthetic. The medical literature supports the fact that COVID patients have increased complications after anesthesia and surgery.
One goal of theanesthesiaconsultant.com is to make the practice of anesthesia safer. The practice of anesthesia on healthy patients is quite safe, but we want to do everything we can to avoid preventable errors. The safety of anesthesia on ASA I and II patients has been compared to the safety record of commercial aviation.
Surgery and anesthesia are never 100% safe, no matter where procedures are done. Large university hospitals staff preoperative anesthesia clinics for their patients, and patients are required to physically visit the clinic to be examined and assessed prior to inpatient surgery. Why Did Take Me So Long To Wake From General Anesthesia?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content